
6
分子診断
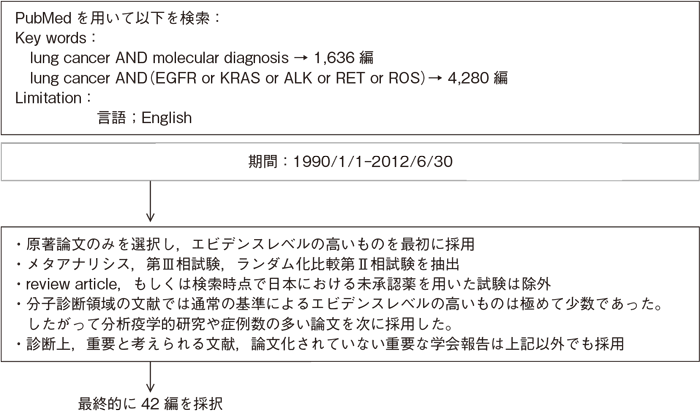
文献検索と採択
6-1.EGFR遺伝子検査
- 推 奨
- a.EGFR遺伝子検査は,非小細胞肺癌におけるEGFR-TKI治療の適応を決定するために行うよう勧められる。(グレードA)
- b.EGFR遺伝子検査は,原則的に腺癌成分を有する組織型において行うよう勧められる。(グレードB)
- c.生検や細胞診などの微量な試料においては,腺癌が含まれない組織型でも,EGFR遺伝子検査を行うことを考慮してよい。(グレードC1)
- d.EGFR遺伝子検査は,確立された高感度法にて行うよう勧められる。(グレードB)
- e.免疫組織化学法(IHC)やコピー数を検出するFISH法は,EGFR-TKI治療の適応を決定するための方法としては勧められない。(グレードD)
*EGFR遺伝子検査に関しては,日本肺癌学会「肺癌患者におけるEGFR遺伝子変異検査の解説」(日本肺癌学会ホームページ:各種ガイドラインhttp//www.haigan.gr.jp)を参照すること。
エビデンス
- a.IPASS試験1)において,臨床背景(組織型,人種,喫煙の有無)ではなく,EGFR遺伝子変異の有無がEGFR-TKIであるゲフィチニブの効果予測因子(ゲフィチニブの抗腫瘍効果は,EGFR変異例で72.1%,EGFR野生型で1.1%)であることが明瞭に示された。またEGFR変異を有する症例のみを対象とした複数の第Ⅲ相試験(WJOG3405試験2)・NEJ002試験3)・OPTIMAL試験4)・EURTAC試験5))において,いずれもEGFR-TKI単剤(ゲフィチニブないしエルロチニブ)がプラチナ製剤併用療法と比較してPFSの有意な延長をもたらすことが報告された。したがってEGFR遺伝子検査は,EGFR-TKI治療の適応を決定するために行うよう勧められる。また,ゲフィチニブ(イレッサ®)においては添付文書上,EGFR遺伝子変異陽性の手術不能または再発非小細胞肺癌患者に投与すること,と規定されており,本検査は必須とされる。
なお,これらの第Ⅲ相臨床試験は,EGFR-TKIと殺細胞性抗癌剤との治療効果のランダム化比較試験としてのエビデンスレベルIIである。IPASS試験は臨床背景で選択した症例を対象にし,他の試験はEGFR遺伝子変異陽性例を対象とした試験であり,EGFR遺伝子変異の有無を層別因子とした比較試験ではない。 - b・c.腺癌以外の組織型,特に扁平上皮癌におけるEGFR変異陽性率は0〜5%と報告されており6)〜10),腺癌と比較すると極めて稀である。さらに手術検体において,免疫染色でΔNp63+/TTF1-をもって扁平上皮癌であることが確認された95症例においては1例もEGFR変異陽性例がなく,当初組織学的に扁平上皮癌と診断されたEGFR変異陽性例10例において,形態および免疫染色による再評価を行ったところ,7例が腺扁平上皮癌,2例が扁平上皮様形態を伴う低分化腺癌で,1例が分類不能であったと報告された11)。したがって,腺癌成分をまったく含まない症例におけるEGFR遺伝子検査は有用でない可能性が高く,腺癌もしくは腺癌組織をわずかでも有する組織型において行うよう勧められる。しかし,生検試料や細胞診試料などの微量なサンプルにおいては,全体像を把握することは困難であり腺癌成分の完全な除外を行うことはできないため,腺癌以外の組織型と診断された症例においても,臨床背景も考慮し,EGFR遺伝子検査を行うことを考慮してもよい。
- d.EGFR遺伝子検査としては,直接塩基配列(ダイレクトシーケンス)法の他,これまでPCRを用いた高感度の検出法を中心として多くの報告がある12)〜17)。検体としては,手術検体,生検検体,気管支洗浄液,胸水,心嚢液,気管支擦過細胞診や吸引細胞診を用いることができるが,特に手術検体以外を検体として用いる場合は,癌細胞含有率が10%以下でも検出できる高感度な検査法が望ましい。検出感度は直接塩基配列法が25%程度とされているのに対し,現在本邦における検査会社で施行可能なPNA-LNA PCR Clamp法12),Scorpion-ARMS法16),Cycleave PCR法15),PCR-invader法17)などは1〜5%で,いずれの方法でも細胞診検体での検出率はほぼ同等であったと報告されており18)19),これらの確立された高感度検出法を用いることが推奨される。
- e.EGFRに対するIHCとしては,全EGFR,リン酸化EGFRあるいは変異特異的EGFRを検出する方法が報告されているが,いずれもEGFR-TKIの効果を予測するには不十分であり,治療の適応を決定するための方法としては勧められない20)〜24)。またEGFR遺伝子コピー数を検出する方法としてFISH(fluorescent in situ hybridization)法やCISH(chromogenic in situ hybridization)法があるが,EGFR遺伝子変異陽性例におけるEGFR-TKIの奏効率が約70%であるのに対して,EGFR遺伝子コピー数増加例のそれは約30%であり,EGFR-TKI治療の適応を決定するための方法としては勧められない20)21)25)26)。
6-2.ALK遺伝子検査
- 推 奨
- a.ALK遺伝子検査は,ALK阻害剤による治療の適否を決定するために行うよう勧められる。(グレードA)
- b.ALK遺伝子検査は,原則的に腺癌成分を有する組織型において行うよう勧められる。(グレードB)
- c.生検や細胞診などの微量な試料においては,腺癌が含まれない組織型でも,ALK遺伝子検査を行うことを考慮してよい。(グレードC1)
- d.ALK遺伝子検査法としては,IHC法,FISH法,RT-PCR法の少なくとも2つ以上の方法によりALK遺伝子の存在を確認することが勧められる。(グレードB)
*ALK遺伝子検査に関しては,日本肺癌学会「肺癌患者におけるALK遺伝子検査の手引き」(日本肺癌学会ホームページ:各種ガイドラインhttp//www.haigan.gr.jp)を参照すること。
エビデンス
- a.ALK遺伝子27)を有する非小細胞肺癌症例に対する,ALK阻害剤であるクリゾチニブの奏効率は61%,PFSは10.0カ月(95%信頼区間8.2〜14.7カ月)と報告され28)29),EGFR遺伝子検査と同様に,ALK遺伝子検査は,ALK阻害剤による治療の適否を決定するために行うよう勧められる。また,ALK阻害剤であるクリゾチニブ(ザーコリ®)の添付文書上,ALK遺伝子陽性が確認された患者に投与すること,と規定されており,本検査は必須とされる。
- b・c.ALK遺伝子においても,EGFR遺伝子変異と同様に扁平上皮癌をはじめ腺癌成分をまったく含まない症例における陽性頻度は極めて低く30)〜36),ALK遺伝子検査は腺癌もしくは腺癌組織をわずかでも有する組織型において行うよう勧められる。ただし,生検試料や細胞診試料などの微量なサンプルにおいては,全体像を把握することは困難であり腺癌成分の完全な除外を行うことはできないため,腺癌以外の組織型と診断された症例においても,臨床背景も考慮し,ALK遺伝子検査を行うことを考慮してもよい。なお,ALK遺伝子とEGFR遺伝子変異とは排他的な関係にあり,同時に異常を有する可能性は極めて低い。したがって,ALK遺伝子検査は,EGFR遺伝子変異陰性例を対象とするなど,状況に応じたALK遺伝子検査を行うことが勧められる。
- d.ALK遺伝子検査としては,FISH法,IHC法,RT-PCR法が報告されている。検体としては,手術検体,生検検体,気管支洗浄液,胸水,心嚢液,気管支擦過細胞診や吸引細胞診検体などを用いることが可能であるが,液性検体ではFISH法あるいはIHC法を施行するためにセルブロックを作成することが推奨される。FISH法については,最も確立された検査法で,これまでの臨床試験においてもALK遺伝子陽性症例の診断根拠として用いられており,標準検査と考えられる28)37)。しかし一方で高価な検査法であり,かつ感度・特異度の面でスクリーニング検査としては不適という指摘もある38)。IHC法については,安価でありスクリーニング検査に適しているが,ALK遺伝子の発現は微量のため通常の染色法では検出が困難であることから,高感度のIHC法が開発されてきた30)32)39)〜41)。したがって,高感度IHC法によりスクリーニングを行い,FISH法により確認を行うことが勧められるが,現時点ではFISH法とIHC法の結果に不一致があることも報告されており,それぞれの結果に基づく治療効果との関連も含めた今後の解析が待たれる。RT-PCR法は既知のALK遺伝子の確認としては確実な方法であるが35),未知の融合遺伝子は検出できないこと,また高品質のRNAが必要なため,通常のホルマリン固定パラフィン包埋標本での解析は困難で,検体採取時点であらかじめRNA用の検体処理を施す必要があることから,現時点では推奨度は低いが,組織採取が困難で気管支洗浄液など細胞診検体しか得られないような症例では有用な可能性がある。以上,それぞれの検査法には長所・短所があり,1つのみの検査法では偽陽性・偽陰性の可能性があることから,得られた検体種に応じてこれらを組み合わせて,2つ以上の方法によりALK遺伝子の存在を確認することが勧められる。
引用文献
- 1)Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009; 361(10): 947-57. (II)
- 2)Mitsudomi T, Morita S, Yatabe Y, et al. Gefitinib versus cisplatin plus docetaxel in patients with non-small-cell lung cancer harbouring mutations of the epidermal growth factor receptor (WJTOG3405): an open label, randomised phase 3 trial. Lancet Oncol. 2010; 11(2): 121-8. (II)
- 3)Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N Engl J Med. 2010; 362(25): 2380-8. (II)
- 4)Zhou C, Wu YL, Chen G, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011; 12(8): 735-42. (II)
- 5)Rosell R, Carcereny E, Gervais R, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012; 13(3): 239-46. (II)
- 6)Marchetti A, Martella C, Felicioni L, et al. EGFR mutations in non-small-cell lung cancer: analysis of a large series of cases and development of a rapid and sensitive method for diagnostic screening with potential implications on pharmacologic treatment. J Clin Oncol. 2005; 23(4): 857-65. (IV)
- 7)Sugio K, Uramoto H, Ono K, et al. Mutations within the tyrosine kinase domain of EGFR gene specifically occur in lung adenocarcinoma patients with a low exposure of tobacco smoking. Br J Cancer. 2006; 94(6): 896-903. (IV)
- 8)Tsao MS, Sakurada A, Ding K, et al. Prognostic and predictive value of epidermal growth factor receptor tyrosine kinase domain mutation status and gene copy number for adjuvant chemotherapy in non-small cell lung cancer. J Thorac Oncol. 2011; 6(1): 139-47. (IV)
- 9)Miyamae Y, Shimizu K, Hirato J, et al. Significance of epidermal growth factor receptor gene mutations in squamous cell lung carcinoma. Oncol Rep. 2011; 25(4): 921-8. (IV)
- 10)Cancer Genome Atlas Research Network. Comprehensive genomic characterization of squamous cell lung cancers. Nature. 2012; 489(7417): 519-25. (IV)
- 11)Rekhtman N, Paik PK, Arcila ME, et al. Clarifying the spectrum of driver oncogene mutations in biomarker-verified squamous carcinoma of lung: lack of EGFR/KRAS and presence of PIK3CA/AKT1 mutations. Clin Cancer Res. 2012; 18(4): 1167-76. (IV)
- 12)Nagai Y, Miyazawa H, Huqun, et al. Genetic heterogeneity of the epidermal growth factor receptor in non-small cell lung cancer cell lines revealed by a rapid and sensitive detection system, the peptide nucleic acid-locked nucleic acid PCR clamp. Cancer Res. 2005; 65(16): 7276-82. (IV)
- 13)Kawada I, Soejima K, Watanabe H, et al. An alternative method for screening EGFR mutation using RFLP in non-small cell lung cancer patients. J Thorac Oncol. 2008; 3(10): 1096-103. (IV)
- 14)Endo K, Konishi A, Sasaki H, et al. Epidermal growth factor receptor gene mutation in non-small cell lung cancer using highly sensitive and fast TaqMan PCR assay. Lung Cancer. 2005; 50(3): 375-84. (IV)
- 15)Yatabe Y, Hida T, Horio Y, et al. A rapid, sensitive assay to detect EGFR mutation in small biopsy specimens from lung cancer. J Mol Diagn. 2006; 8(3): 335-41. (IV)
- 16)Kimura H, Fujiwara Y, Sone T, et al. High sensitivity detection of epidermal growth factor receptor mutations in the pleural effusion of non-small cell lung cancer patients. Cancer Sci. 2006; 97(7): 642-8. (IV)
- 17)Naoki K, Soejima K, Okamoto H, et al. The PCR-invader method (structure-specific 5' nuclease-based method), a sensitive method for detecting EGFR gene mutations in lung cancer specimens; comparison with direct sequencing. Int J Clin Oncol. 2011; 16(4): 335-44. (IV)
- 18)Pao W, Ladanyi M. Epidermal growth factor receptor mutation testing in lung cancer: searching for the ideal method. Clin Cancer Res. 2007; 13(17): 4954-5. (IV)
- 19)Goto K, Satouchi M, Ishii G, et al. An evaluation study of EGFR mutation tests utilized for non-small-cell lung cancer in the diagnostic setting. Ann Oncol. 2012; 23(11): 2914-9. (IV)
- 20)Miller VA, Riely GJ, Zakowski MF, et al. Molecular characteristics of bronchioloalveolar carcinoma and adenocarcinoma, bronchioloalveolar carcinoma subtype, predict response to erlotinib. J Clin Oncol. 2008; 26(9): 1472-8. (IV)
- 21)Sholl LM, Xiao Y, Joshi V, et al. EGFR mutation is a better predictor of response to tyrosine kinase inhibitors in non-small cell lung carcinoma than FISH, CISH, and immunohistochemistry. Am J Clin Pathol. 2010; 133(6): 922-34. (IV)
- 22)Yu J, Kane S, Wu J, et al. Mutation-specific antibodies for the detection of EGFR mutations in non-small-cell lung cancer. Clin Cancer Res. 2009; 15(9): 3023-8. (IV)
- 23)Kawahara A, Yamamoto C, Nakashima K, et al. Molecular diagnosis of activating EGFR mutations in non-small cell lung cancer using mutation-specific antibodies for immunohistochemical analysis. Clin Cancer Res. 2010; 16(12): 3163-70. (IV)
- 24)Kato Y, Peled N, Wynes MW, et al. Novel epidermal growth factor receptor mutation-specific antibodies for non-small cell lung cancer: immunohistochemistry as a possible screening method for epidermal growth factor receptor mutations. J Thorac Oncol. 2010; 5(10): 1551-8. (IV)
- 25)Zhu CQ, da Cunha Santos G, Ding K, et al. Role of KRAS and EGFR as biomarkers of response to erlotinib in National Cancer Institute of Canada Clinical Trials Group Study BR.21. J Clin Oncol. 2008; 26(26): 4268-75. (IV)
- 26)Hirsch FR, Kabbinavar F, Eisen T, et al. A randomized, phase II, biomarker-selected study comparing erlotinib to erlotinib intercalated with chemotherapy in first-line therapy for advanced non-small-cell lung cancer. J Clin Oncol. 2011; 29(26): 3567-73. (III)
- 27)Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007; 448(7153): 561-6. (IV)
- 28)Kwak EL, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010; 363(18): 1693-703. (IV)
- 29)Camidge DR, Bang YJ, Kwak EL, et al. Progression-free survival (PFS) from a phase I study of crizotinib (PF-02341066) in patients with ALK-positive non-small cell lung cancer (NSCLC). J Clin Oncol. 2011; 29(15): 2501. (IV)
- 30)Boland JM, Erdogan S, Vasmatzis G, et al. Anaplastic lymphoma kinase immunoreactivity correlates with ALK gene rearrangement and transcriptional up-regulation in non-small cell lung carcinomas. Hum Pathol. 2009; 40(8): 1152-8. (IV)
- 31)Inamura K, Takeuchi K, Togashi Y, et al. EML4-ALK fusion is linked to histological characteristics in a subset of lung cancers. J Thorac Oncol. 2008; 3(1): 13-7. (IV)
- 32)Inamura K, Takeuchi K, Togashi Y, et al. EML4-ALK lung cancers are characterized by rare other mutations, a TTF-1 cell lineage, an acinar histology, and young onset. Mod Pathol. 2009; 22(4): 508-15. (IV)
- 33)Koivunen JP, Mermel C, Zejnullahu K, et al. EML4-ALK fusion gene and efficacy of an ALK kinase inhibitor in lung cancer. Clin Cancer Res. 2008; 14(13): 4275-83. (IV)
- 34)Salido M, Pijuan L, Martínez-Avilés L, et al. Increased ALK gene copy number and amplification are frequent in non-small cell lung cancer. J Thorac Oncol. 2011; 6(1): 21-7. (IV)
- 35)Takeuchi K, Choi YL, Soda M, et al. Multiplex reverse transcription-PCR screening for EML4-ALK fusion transcripts. Clin Cancer Res. 2008; 14(20): 6618-24. (IV)
- 36)Takahashi T, Sonobe M, Kobayashi M, et al. Clinicopathologic features of non-small-cell lung cancer with EML4-ALK fusion gene. Ann Surg Oncol. 2010; 17(3): 889-97. (IV)
- 37)Camidge DR, Kono SA, Flacco A, et al. Optimizing the detection of lung cancer patients harboring anaplastic lymphoma kinase (ALK) gene rearrangements potentially suitable for ALK inhibitor treatment. Clin Cancer Res. 2010; 16(22): 5581-90. (IV)
- 38)Chihara D, Suzuki R. More on crizotinib. N Engl J Med. 2011; 364(8): 776-7. (VI)
- 39)Takeuchi K, Choi YL, Togashi Y, et al. KIF5B-ALK, a novel fusion oncokinase identified by an immunohistochemistry-based diagnostic system for ALK-positive lung cancer. Clin Cancer Res. 2009; 15(9): 3143-9. (IV)
- 40)Mino-Kenudson M, Chirieac LR, Law K, et al. A novel, highly sensitive antibody allows for the routine detection of ALK-rearranged lung adenocarcinomas by standard immunohistochemistry. Clin Cancer Res. 2010; 16(5): 1561-71. (IV)
- 41)Paik JH, Choe G, Kim H, et al. Screening of anaplastic lymphoma kinase rearrangement by immunohistochemistry in non-small cell lung cancer: correlation with fluorescence in situ hybridization. J Thorac Oncol. 2011; 6(3): 466-72. (IV)
