
2
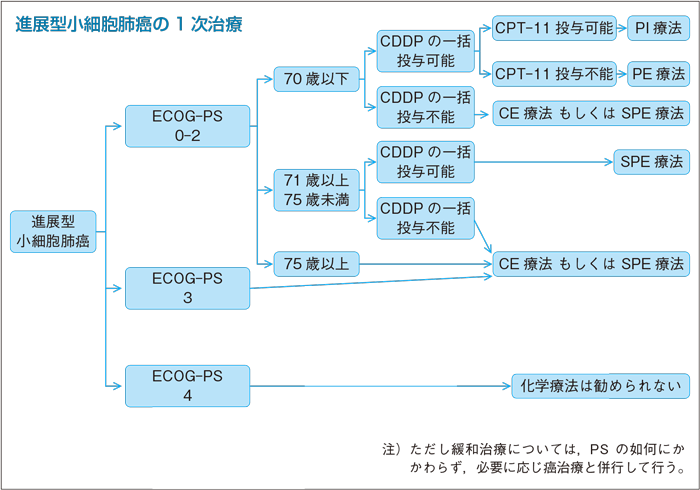
進展型小細胞肺癌の一次治療
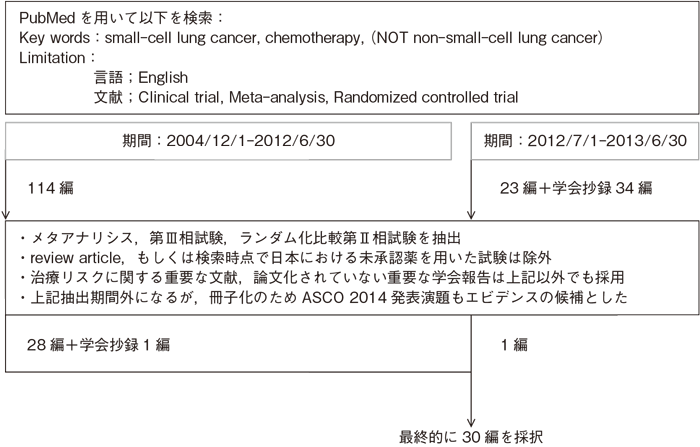
文献検索と採択
本文中に用いた略語および用語の解説
| AMR | アムルビシン | ETP | エトポシド |
| CBDCA | カルボプラチン | GEM | ゲムシダビン |
| CDDP | シスプラチン | PTX | パクリタキセル |
| CPA | シクロフォスファミド | VCR | ビンクリスチン |
| CPT-11 | イリノテカン | VNR | ビノレルビン |
| DXR | ドキソルビシン | プラチナ製剤 | CDDPとCBDCAの総称 |
| ACE | ドキソルビシン+シクロフォスファミド+エトポシド | |
| CAV | シクロフォスファミド+ドキソルビシン+ビンクリスチン | |
| CE | カルボプラチン+エトポシド | |
| PA | シスプラチン+アムルビシン | |
| PE | シスプラチン+エトポシド | |
| PI | シスプラチン+イリノテカン | |
| SPE | 分割投与シスプラチン+エトポシド | |
| ECOG | Eastern Cooperative Oncology Group | 米国東海岸癌臨床試験グループ |
| JCOG | Japan Clinical Oncology Group | 日本臨床腫瘍研究グループ |
| PCI | prophylactic cranial irradiation | 予防的全脳照射 |
| PS | performance status | 一般状態 |
| SCLC | small cell lung cancer | 小細胞肺癌 |
樹形図
補足:小細胞肺癌の限局型(Limited Disease;LD)および進展型(Extensive disease;ED)の定義について
肺癌取扱い規約第7版(日本肺癌学会編)では小細胞肺癌について,「limited disease」(限局型)と「extensive disease」(進展型)の分類には意見の一致が得られておらず,「limited」と「extensive」の定義が確立していない現状では,TNMの記載は重要であるとしている。
しかし,小細胞肺癌の治療選択の面からは,限局型と進展型の区分は重要と考えられるため,本ガイドラインでは多くの第Ⅲ相臨床試験で採用されている定義,すなわち病変が同側胸郭内に加え,対側縦隔,対側鎖骨上窩リンパ節までに限られており悪性胸水,心嚢水を有さないものを限局型小細胞肺癌と定義付けた。
しかし,小細胞肺癌の治療選択の面からは,限局型と進展型の区分は重要と考えられるため,本ガイドラインでは多くの第Ⅲ相臨床試験で採用されている定義,すなわち病変が同側胸郭内に加え,対側縦隔,対側鎖骨上窩リンパ節までに限られており悪性胸水,心嚢水を有さないものを限局型小細胞肺癌と定義付けた。
ECOG(Eastern Cooperative Oncology Group) Performance Status
| PS | |
|---|---|
| 0 | 無症状で社会活動ができ,制限を受けることなく発病前と同等に振る舞える。 |
| 1 | 軽度の症状があり,肉体労働は制限を受けるが,歩行,軽労働や座業はできる。例えば軽い家事,事務など。 |
| 2 | 歩行や身の回りのことはできるが,時に少し介助がいることもある。軽労働はできないが,日中の50%以上は起居している。 |
| 3 | 身の回りのある程度のことはできるが,しばしば介助がいり,日中の50%以上は就床している。 |
| 4 | 身の回りのこともできず,常に介助がいり,終日就床を必要としている。 |
2-1.進展型小細胞肺癌の1次治療
- 推 奨
- a.PS 0-3の進展型小細胞肺癌に対する化学療法は,プラチナ製剤を含む併用化学療法を行うよう勧められる。
- a-1.70歳以下のPS 0-2の患者にはシスプラチン+イリノテカンが推奨される。(グレードA)
- a-2.71歳以上75歳未満のPS 0-2患者および70歳以下でイリノテカンの毒性が懸念される患者にはシスプラチン+エトポシドが推奨される。(グレードA)
- a-3.下記の患者にはシスプラチン分割もしくはカルボプラチン+エトポシドが推奨される。(グレードB)
- ・PS 0-2でシスプラチンの一括投与ができない
- ・75歳以上
- ・PS 3
- b.進展型小細胞肺癌に対する初回治療は4コース行うよう勧められる。(グレードA)
- c.維持療法の有用性は認められておらず,行うよう勧めるだけの根拠が明確でない。(グレードC2)
- d.大量化学療法あるいは単位時間あたりの投与量を増やし,治療強度を高めた化学療法は行わないよう勧められる。(グレードD)
- e.化学療法後のPCIは行わないよう勧められる。(グレードD)
エビデンス
- a.1960年代,進展型小細胞肺癌患者を対象に行われたシクロフォスファミド(CPA)単剤と緩和治療(BSC;best supportive care)との比較試験で,化学療法群の生存期間が約2倍に延長することが示された1)。1970年代にはCPA単剤と多剤併用化学療法との比較試験が行われ,多剤併用化学療法での生存期間延長が示された2)〜4)。1970〜80年代はCPAを含む併用化学療法が広く用いられていたが,1980年代以降CDDP+ETP(PE)との比較試験が行われた。2000年に報告されたCCDPを含む化学療法とそれ以外との比較試験のメタアナリシスでは,CDDPを含むレジメンが奏効率および1年生存率が有意に高く,治療関連死には差を認めなかったとしている5)。2000年以降世界的にはPEが標準治療と考えられてきた。2008年にはプラチナ製剤を含む化学療法とそれ以外とのメタアナリシスが行われ,全生存期間,奏効率に差はなく,プラチナ併用群で悪心・嘔吐,貧血,血小板減少が多く,完全寛解率が高かったと報告された6)。PEとDXR+CPA+ETP(ACE)との比較試験では,奏効率,生存期間に有意差はなく,ACEが有意に好中球減少,敗血症の割合が高かったことが示されている7)。
- a-1.本邦で行われた70歳以下のPS 0-2を対象とした,PEとCDDP+CTP-11(PI)との比較試験(JCOG9511)の結果,PIが有意に生存期間を延長することが示された(生存期間中央値9.4カ月 vs 12.8カ月)8)。その後,北米を中心にPEとPIとの比較試験の追試が行われたが,JCOG9511の結果を再現することはできなかった9)〜11)。しかし,プラチナ製剤+ETPとプラチナ製剤+CPT-11とのランダム化試験のメタアナリシスでは,CPT-11群が有意に奏効率が高く,生存期間を延長し,血液毒性が軽度で,嘔吐,下痢の頻度が高いことが示されている12)〜14)。PIとCDDP+AMR(PA)との比較試験が本邦で行われ,PAはPIに対する非劣性を証明することはできなかった(生存期間中央値15.0カ月 vs 18.3カ月)15)。これらの結果から,JCOG9511の対象となったPS 0-2の70歳以下の患者にはPIが推奨される。
- a-2.1980年代以降PEは小細胞肺癌の治療に頻用され,海外の第Ⅲ相試験では年齢制限なく臨床試験が行われていることが多い。日本では75歳未満のPS 0-3の小細胞肺癌(限局型,進展型を含む)に対しPEとCPA+DXR+VCR(CAV)とCAV/PE交代療法を比較する第Ⅲ相試験が行われ,PE療法とCAV/PE療法の奏効率がCAVより有意に高く,毒性は許容範囲であった16)。PIに関して,71歳以上の高齢者の小細胞肺癌に対する本邦のエビデンスは現時点では存在しない。しかしながら,非小細胞肺癌に対する治療としてもCDDP+CPT-11は使用されており,日本において74歳までのPS 0-1の進行期非小細胞肺癌を対象にCDDP+CPT-11,CDDP+GEM,CDDP+VCR,CBDCA+DTXの4群を比較する第Ⅲ相試験17)の結果より毒性は許容範囲であることから,実地臨床では74歳までの小細胞肺癌に使用されることもある。また,1つの第Ⅲ相試験のサブセット解析のみであるが,CDDPを含む併用化学療法のランダム化試験に参加した70歳以上の高齢者の解析では,若年者との比較で明らかな差は認めていないとの報告もある18)。CPT-11は下痢が臨床的に問題であり,また間質性肺炎を有する患者には禁忌とされている。そのため,下痢の発症が懸念される患者にはPEが推奨され,間質性肺炎の発症が懸念される患者にはPEが選択肢になる。
- a-3.JCOGは,70歳以上かつPS 0-2の高齢者および70歳以下のPS 3の患者を対象にsplit PE(SPE:CDDP 3日間分割投与)とCBDCA+ETP(CE)との比較試験を行い,CE群で血小板減少が多く,奏効率,生存期間はほぼ同様であった(JCOG9702)19)。本邦で行われたPS 3に対する治療効果に関するエビデンスはJCOG9702のサブセット解析のみである。CDDPの毒性が懸念される患者に対しては,CBDCAを用いることも推奨される。また,海外の試験でも,約15%のPS 3を含めた第Ⅲ相試験20)もあり,いずれもサブセット解析のみではあるが,PS 3に関しては小細胞肺癌に対する治療効果によってPSの改善が得られる可能性があれば化学療法の対象になり得る。PS 4を含めた第Ⅲ相試験21)もあるが,PS 4の登録は3%とごくわずかである。PS 4を主たる対象にしての前向き試験の評価は行われておらず,進展型小細胞癌に関するエビデンスはないのが現状である。
- b・c.治療期間に関し,維持療法を含めたメタアナリシスで長期化学療法が予後を延長したとする報告がある22)。しかし,これらはかなり古い試験の解析であり,現在用いられている薬剤は少ない。最近報告されたCPT-11を用いた維持療法のランダム化試験では明らかな差は認めておらず23),現時点で維持療法は推奨されない。PI,PEを用いた臨床試験の多くは投与コース数を4コースとしていることより投与コース数は4コースが推奨される。a-3で述べたPE(3日間分割投与)とCBDCA+ETP(CE)との比較試験(JCOG9702)においても投与コース数は4コースとされている。
- d.大量化学療法あるいは治療強度を高めた治療法に関しては,最近の報告でも有用性を示したものはなく,一般診療では行わないよう勧められる24)〜28)。
- e.Auperinらは1977年から1995年までの7つの臨床試験登録例のうち,完全寛解(CR)*に至った987例のメタアナリシスを行い29),PCIが3年生存率を15.3%から20.7%へと有意に向上させることを報告した。このうち進展型症例のサブセットは140例(14%)と少数で,生存期間延長の傾向が認められたものの有意ではなかった。また,解析に含まれた試験の中でCR判定を胸部単純X線のみで行ったものがいくつか存在しており,現在の日常臨床からすると不十分な評価であった可能性がある。
その後,Slotmanらは進展型小細胞癌で初期治療に反応した症例(PR症例が87%)に対するランダム化比較試験を行い30),PCIにより生存期間中央値が約1カ月延長すること(6.7カ月 vs 5.4カ月,P=0.003)を報告した。しかしながら,この試験では登録前に脳転移の有無を確認されたものが29%にとどまっているなど,試験デザインの問題が指摘されていた。
2014年に,本邦で行われた第Ⅲ相試験の結果が報告された。プラチナ併用初回化学療法後に奏効した脳転移のない進展型小細胞癌に対するPCI施行群とPCI未施行群との比較試験である31)。転移性脳腫瘍の12カ月間の出現頻度は,32.4%と58.0%と有意に減少したが,主要評価項目であるOSは中間解析の結果,10.1カ月と15.1カ月(HR 1.38, 95%CI:0.95-2.02, P=0.091)であり,早期無効中止となった。今回の試験結果を踏まえ,本邦においては,PCIを追加する意義はなく,推奨グレードをDとした。
*CR:すべての標的病変,非標的病変が消失した場合。
引用文献
- 1)Green RA, Humphrey E, Close H, et al. Alkylating agents in bronchogenic carcinoma. Am J Med. 1969; 46(4): 516-25. (II)
- 2)Edmonson JH, Lagakos SW, Selawry OS, et al. Cyclophosphamide and CCNU in the treatment of inoperable small cell carcinoma and adenocarcinoma of the lung. Cancer Treat Rep. 1976; 60(7): 925-32. (II)
- 3)Alberto P, Brunner KW, Martz G, et al. Treatment of bronchogenic carcinoma with simultaneous or sequential combination chemotherapy, including methotrexate, cyclophosphamide, procarbazine and vincristine. Cancer. 1976; 38(6): 2208-16. (II)
- 4)Lowenbraun S, Bartolucci A, Smalley RV, et al. The superiority of combination chemotherapy over single agent chemotherapy in small cell lung carcinoma. Cancer. 1979; 44(2): 406-13. (II)
- 5)Pujol JL, Carestia L, Daurès JP. Is there a case for cisplatin in the treatment of small-cell lung cancer? A meta-analysis of randomized trials of a cisplatin-containing regimen versus a regimen without this alkylating agent. Br J Cancer. 2000; 83(1): 8-15. (I)
- 6)Amarasena IU, Walters JA, Wood-Baker R, et al. Platinum versus non-platinum chemotherapy regimens for small cell lung cancer. Cochrane Database Syst Rev. 2008; (4): CD006849. (I)
- 7)Baka S, Califano R, Ferraldeschi R, et al. Phase III randomised trial of doxorubicin-based chemotherapy compared with platinum-based chemotherapy in small-cell lung cancer. Br J Cancer. 2008; 99(3): 442-7. (II)
- 8)Noda K, Nishiwaki Y, Kawahara M, et al. Irinotecan plus cisplatin compared with etoposide plus cisplatin for extensive small-cell lung cancer. N Engl J Med. 2002; 346(2): 85-91. (II)
- 9)Hanna N, Bunn PA Jr, Langer C, et al. Randomized phase III trial comparing irinotecan/cisplatin with etoposide/cisplatin in patients with previously untreated extensive-stage disease small-cell lung cancer. J Clin Oncol. 2006; 24(13): 2038-43. (II)
- 10)Lara PN Jr, Natale R, Crowley J, et al. Phase III trial of irinotecan/cisplatin compared with etoposide/cisplatin in extensive-stage small-cell lung cancer: clinical and pharmacogenomic results from SWOG S0124. J Clin Oncol. 2009; 27(15): 2530-5. (II)
- 11)Zatloukal P, Cardenal F, Szczesna A, et al. A multicenter international randomized phase III study comparing cisplatin in combination with irinotecan or etoposide in previously untreated small-cell lung cancer patients with extensive disease. Ann Oncol. 2010; 21(9): 1810-6. (II)
- 12)Jiang L, Yang KH, Mi DH, et al. Safety of irinotecan/cisplatin versus etoposide/cisplatin for patients with extensive-stage small-cell lung cancer: a metaanalysis. Clin Lung Cancer. 2007; 8(8): 497-501. (I)
- 13)Jiang J, Liang X, Zhou X, et al. A meta-analysis of randomized controlled trials comparing irinotecan/platinum with etoposide/platinum in patients with previously untreated extensive-stage small cell lung cancer. J Thorac Oncol. 2010; 5(6): 867-73. (I)
- 14)Lima JP, dos Santos LV, Sasse EC, et al. Camptothecins compared with etoposide in combination with platinum analog in extensive stage small cell lung cancer: systematic review with meta-analysis. J Thorac Oncol. 2010; 5(12): 1986-93. (I)
- 15)Satouchi M, Kotani Y, Shibata T, et al. Phase III study comparing amrubicin plus cisplatin with irinotecan plus cisplatin in the treatment of extensive-disease small-cell lung cancer: JCOG 0509. J Clin Oncol. 2014; 32(12): 1262-8.
- 16)Fukuoka M, Furuse K, Saijo N, et al. Randomized trial of cyclophosphamide, doxorubicin, and vincristine versus cisplatin and etoposide versus alternation of these regimens in small-cell lung cancer. J Natl Cancer Inst. 1991; 83(12): 855-61. (II)
- 17)Ohe Y, Ohashi Y, Kubota K, et al. Randomized phase III study of cisplatin plus irinotecan versus carboplatin plus paclitaxel, cisplatin plus gemcitabine, and cisplatin plus vinorelbine for advanced non-small-cell lung cancer: Four-Arm Cooperative Study in Japan. Ann Oncol. 2007; 18(2): 317-23. (II)
- 18)Safont MJ, Artal-Cortes A, Sirera R, et al. Retrospective study of efficacy and toxicity on patients older than 70 years within a randomized clinical trial of two cisplatin-based combinations in patients with small-cell lung cancer. Lung Cancer. 2009; 63(1): 83-7. (III)
- 19)Okamoto H, Watanabe K, Kunikane H, et al. Randomised phase III trial of carboplatin plus etoposide vs split doses of cisplatin plus etoposide in elderly or poor-risk patients with extensive disease small-cell lung cancer: JCOG 9702. Br J Cancer. 2007; 97(2): 162-9. (II)
- 20)Souhami RL, Spiro SG, Rudd RM, et al. Five-day oral etoposide treatment for advanced small-cell lung cancer: randomized comparison with intravenous chemotherapy. J Natl Cancer Inst. 1997; 89(8): 577-80. (II)
- 21)Girling DJ. Comparison of oral etoposide and standard intravenous multidrug chemotherapy for small-cell lung cancer: a stopped multicentre randomised trial. Medical Research Council Lung Cancer Working Party. Lancet. 1996; 348(9027): 563-6. (II)
- 22)Bozcuk H, Artac M, Ozdogan M, et al. Does maintenance/consolidation chemotherapy have a role in the management of small cell lung cancer (SCLC)? A metaanalysis of the published controlled trials. Cancer. 2005; 104(12): 2650-7. (I)
- 23)Han JY, Kim HT, Lim KY, et al. Randomized phase II study of maintenance irinotecan therapy versus observation following induction chemotherapy with irinotecan and cisplatin in extensive disease small cell lung cancer. J Thorac Oncol. 2008; 3(9): 1039-45. (II)
- 24)Lorigan P, Woll PJ, O'Brien ME, et al. Randomized phase III trial of dose-dense chemotherapy supported by whole-blood hematopoietic progenitors in better-prognosis small-cell lung cancer. J Natl Cancer Inst. 2005; 97(9): 666-74. (II)
- 25)Buchholz E, Manegold C, Pilz L, et al. Standard versus dose-intensified chemotherapy with sequential reinfusion of hematopoietic progenitor cells in small cell lung cancer patients with favorable prognosis. J Thorac Oncol. 2007; 2(1): 51-8. (II)
- 26)Leyvraz S, Pampallona S, Martinelli G, et al; Solid Tumors Working Party of the European Group for Blood and Marrow Transplantation. A threefold dose intensity treatment with ifosfamide, carboplatin, and etoposide for patients with small cell lung cancer: a randomized trial. J Natl Cancer Inst. 2008; 100(8): 533-41. (II)
- 27)Heigener DF, Manegold C, Jäger E, et al. Multicenter randomized open-label phase III study comparing efficacy, safety, and tolerability of conventional carboplatin plus etoposide versus dose-intensified carboplatin plus etoposide plus lenograstim in small-cell lung cancer in "extensive disease" stage. Am J Clin Oncol. 2009; 32(1): 61-4. (II)
- 28)Jiang J, Shi HZ, Deng JM, et al. Efficacy of intensified chemotherapy with hematopoietic progenitors in small-cell lung cancer: A meta-analysis of the published literature. Lung Cancer. 2009; 65(2): 214-8. (I)
- 29)Aupérin A, Arriagada R, Pignon JP, et al. Prophylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic Cranial Irradiation Overview Collaborative Group. N Engl J Med. 1999; 341(7): 476-84. (I)
- 30)Slotman B, Faivre-Finn C, Kramer G, et al; EORTC Radiation Oncology Group and Lung Cancer Group. Prophylactic cranial irradiation in extensive small-cell lung cancer. N Engl J Med. 2007; 357(7): 664-72. (II)
- 31)Seto T, Takahashi T, Yamanaka T, et al. Prophylactic cranial irradiation (PCI) has a detrimental effect on the overall survival (OS) of patients (pts) with extensive disease small cell lung cancer (ED-SCLC): Results of a Japanese randomized phase III trial. J Clin Oncol. 2012; 32: suppl. abstract 7503. (II)
進展型小細胞肺癌レジメン
| PI療法 | |||
| CDDP | 60mg/m2, on day 1 | ||
| CPT-11 | 60mg/m2, on day 1, 8, 15 | q4w | |
| PE療法 | |||
|---|---|---|---|
| CDDP | 80mg/m2, on day 1 | ||
| ETP | 100mg/m2, on day 1, 2, 3 | q3w | |
| CE療法 | |||
| CBDCA | AUC=5, on day 1 | ||
| ETP | 80mg/m2, on day 1, 2, 3 | q3〜4w | |
| SPE(CDDP分割)療法 | |||
| CDDP | 25mg/m2, on day 1, 2, 3 | ||
| ETP | 80mg/m2, on day 1, 2, 3 | q3〜4w | |
