
1
危険因子と臨床症状,検出方法
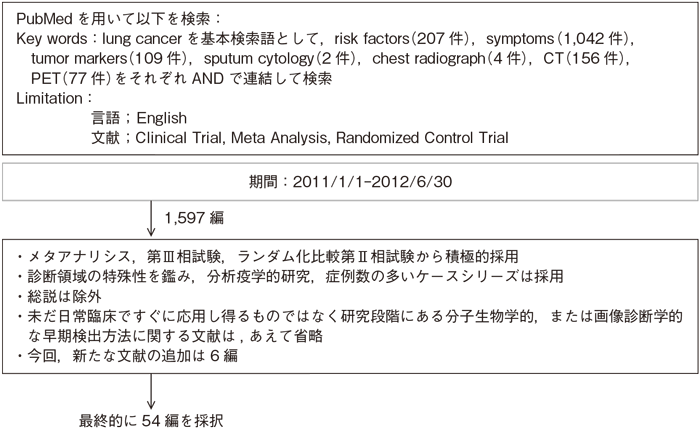
文献検索と採択
1-1.危険因子と臨床症状
- 推 奨
- 危険因子例・有症状例に対しては肺癌検出のための検査を行うよう勧められる。(グレードA)
- a.危険因子:喫煙の他に慢性閉塞性肺疾患,アスベスト症などの吸入性肺疾患,肺癌の既往歴や家族歴,年齢,肺結核など
- b.肺癌にみられる症状:咳嗽,喀痰,血痰,発熱,呼吸困難,胸痛といった呼吸器症状および転移病巣による症状
エビデンス
- a.肺癌の発生率は50歳以上で急激に増加する。日本人が生涯のうちに肺癌になる割合は男で7.4%,女で3.1%である1)。非喫煙者に比べて,喫煙者が肺癌になるリスクは男で4.4倍,女で2.8倍と高い2)。喫煙開始年齢が若いほど喫煙量が多いほど肺癌リスクは高い3)4)。喫煙者が禁煙すると,喫煙を継続した場合に比較して肺癌リスクが低下し,禁煙年齢が低いほど,その効果が大きい5)。受動喫煙の曝露を受けた者はそうでない者に比べて肺癌リスクは約1.3倍に増加する3)6)。喫煙以外に,慢性閉塞性肺疾患(肺気腫,慢性気管支炎),職業的曝露(アスベスト,ラドン,ヒ素,クロロメチルエーテル,クロム酸,ニッケル),大気汚染(特に粒径2.5ミクロン以下の微小浮遊粒子),肺癌の既往歴や家族歴,年齢なども肺癌リスクを高めると報告されている7)〜10)。また,肺結核の診断後2年以内の肺癌リスクは約5.0倍に増加し,その後も約1.5倍から3.3倍の肺癌リスクが持続するとの報告もある11)〜13)。
- b.肺癌に特徴的な臨床症状はないが,多くの患者は,咳嗽,喀痰,血痰,発熱,呼吸困難,胸痛といった呼吸器症状をきっかけに発見される。症状発見の肺癌は,検診発見の肺癌と比較すると,進行肺癌の頻度が高く,予後が悪いと報告されている14)〜17)。
臨床検査所見も非特異的であるが,腫瘍に随伴する異常所見や転移に伴う異常所見を検出するために,血球数,電解質,カルシウム,アルカリホスファターゼ,肝酵素を含む生化学検査が必要である18)。
1-2.検出方法
- 推 奨
- 危険因子例・有症状例に対して肺癌を疑う場合の検出方法には,胸部X線写真,胸部CT,喀痰細胞診などがあり,組み合わせて用いることが勧められる。(グレードA)
- a.胸部X線写真は,肺癌検出を目的として,最初に行うよう勧められる。(グレードA)
- b.胸部CTは,肺癌検出を目的として,あるいは胸部X線写真で異常がある場合に,行うよう勧められる。(グレードA)
- c.喀痰細胞診は,中心型早期肺癌の検出を目的として,行うよう勧められる。(グレードA)
- d.腫瘍マーカーおよびPET/CTは,肺癌検出の目的としては,行うよう勧められない。(グレードD)
エビデンス
- a.胸部X線写真は,簡便で広く普及した検査法である。日常診療において,胸部X線写真による肺癌の検出感度は,80%程度と報告されている19)。検診発見の臨床病期Ⅰ期の肺野型腺癌の58%が2年前のX線写真でも描出されていたという報告もみられる20)。その要因として,病変が小さく淡いこと,正常構造に重なっていることなどが挙げられる21)22)。特に肺胞置換型発育をする淡い小型腺癌の検出率は23%にとどまる23)。また,読影には熟練も関係することが報告されている24)。
- b.胸部CTは,臨床的に問題となる大きさの肺癌を検出する形態診断法として,現時点で最も有力な検査である25)〜27)。病変の有無を検索する従来型CTでは,肺野結節の検出能は病変の大きさに依存し,6mm以上の大きさの結節では95%の検出能が得られるが,6mm以下の結節では70%程度に低下し,特に3mm以下では検出能が低下する25)。大きさ以外の見落としの要因としては,気管支内病変,淡い病変,血管構造に近接する病変などが挙げられ,読影者側の要因も存在する28)〜30)。また,ヘリカルCTは,従来型CTよりも検出率が向上する31)。限局性のすりガラス陰影を呈する肺癌は,CTのみで発見される場合が多い。
- c.喀痰細胞診は,非侵襲的で簡便に行える中心型早期肺癌の唯一のスクリーニング法である。肺癌症例における喀痰細胞診の検出感度は36〜40%にすぎない32)〜34)が,喀痰細胞診で発見されたX線陰性肺癌は長期生存例の割合が高いことも報告されている35)。また,喀痰細胞診を胸部X線写真に追加するスクリーニング法の有効性を検討したランダム化比較試験であるJohns Hopkins Study36)とMemorial Sloan-Kettering Study37)では,喀痰細胞診を追加するグループにおいて早期癌の割合,切除率,5年生存率が上昇することが示された。肺癌死亡率の減少効果に関しても,両studyを長期追跡した混合解析の結果,有意差はないものの死亡率を12%低下させる傾向が認められた38)。
- d. 腫瘍マーカーを用いた肺癌検出率は,対象集団の事前確率に影響されるため,一般集団を対象に感度と特異度の優れた腫瘍マーカーを検査しても肺癌検出率は向上しないことが示されている39)。また,腫瘍マーカーは非腫瘍性疾患でも上昇することが広く知られている。非小細胞癌症例に対する検出感度はCYFRA21-1が41〜65%であり,CEA,SLX,CA19-9,CA125,SCC,TPAの感度はCYFRA21-1よりも低い40)〜45)。また小細胞癌症例に対する検出感度はNSEが47%,ProGRPが45%46)程度である。CEA,CYFRA21-1,ProGRP,NSEなどの腫瘍マーカーの変動は腫瘍の病期あるいは治療効果と良好に相関することが報告されている47)〜50)。したがって,腫瘍マーカーは肺癌検出の目的ではなく,肺癌の質的診断の補助,治療効果のモニタリング,再発診断の補助として行うよう勧められる。
胸部CTで検出可能な肺悪性結節のPET/CTによる検出感度は約70%であり,直径10mm未満や低い組織学的グレードの肺悪性結節はPET/CTで偽陰性を呈しやすいことが示されている51)52)。また,PET/CTは非腫瘍性疾患でも偽陽性を呈することが広く知られている。一方,肺結節の良悪性鑑別に対するPET/CTの正診率は,メタアナリシスの結果,有意差はないもののPET/CTが胸部X線CTよりも優れる傾向性が認められた53)54)。したがって,PET/CTは肺癌検出の目的ではなく,肺結節の質的診断の補助として行うよう勧められる。
引用文献
1-1.危険因子と臨床症状
a.危険因子
a.危険因子
- 1)加茂憲一,金子聡,吉村公雄,他.日本人におけるがん生涯リスク評価.厚生の指標,2005; 52(6): 21-6. (IV)
- 2)Wakai K, Inoue M, Mizoue T, et al; Research Group for the Development and Evaluation of Cancer Prevention Strategies in Japan. Tobacco smoking and lung cancer risk: an evaluation based on a systematic review of epidemiological evidence among the Japanese population. Jpn J Clin Oncol. 2006; 36: 309-24. (IV)
- 3)Tobacco Smoke and Involuntary Smoking, IARC Monographs Volume 83 (2004)(IV)
- 4)A Report of the Surgeon General, The Health Consequences of Smoking (2004)(IV)
- 5)Tobacco Control: Reversal of Risk after Quitting Smoking, IARC Handbook of Cancer Prevention, Volume 11 (2007)(IV)
- 6)A Report of the Surgeon General, The Health Consequences of Involuntary Exposure to Tobacco Smoke (2006)(IV)
- 7)Spitz MR, Wu X, Wilkinson A, et al. Cancer of the lung. In : Shottenfelt D. Fraumeni JF eds. "Cancer Epidemiology and Prevention 3rd ed." pp638-658 Oxford University Press (2006)(IV)
- 8)Wang H, Yang L, Zou L, et al. Association between chronic obstructive pulmonary disease and lung cancer: a case-control study in Southern Chinese and a meta-analysis. PLoS One. 2012; 7(9): e46144. (I)
- 9)Smith BM, Pinto L, Ezer N, et al. Emphysema detected on computed tomography and risk of lung cancer: a systematic review and meta-analysis. Lung Cancer. 2012; 77(1): 58-63. (IV)
- 10)'t Mannetje A, Bencko V, Brennan P, et al. Occupational exposure to metal compounds and lung cancer. Results from a multi-center case-control study in Central/Eastern Europe and UK. Cancer Causes Control. 2011; 22(12): 1669-80. (IV)
- 11)Brenner DR, McLaughlin JR, Hung RJ. Previous lung diseases and lung cancer risk: a systematic review and meta-analysis. PLoS One. 2011; 6(3):e17479. (I)
- 12)Yu YH, Liao CC, Hsu WH, et al. Increased lung cancer risk among patients with pulmonary tuberculosis: a population cohort study. J Thorac Oncol. 2011; 6(1): 32-7. (IV)
- 13)Shiels MS, Albanes D, Virtamo J, et al. Increased risk of lung cancer in men with tuberculosis in the alpha-tocopherol, beta-carotene cancer prevention study. Cancer Epidemiol Biomarkers Prev. 2011; 20(4): 672-8. (IV)
b.肺癌にみられる症状
- 14)Shimizu N, Ando A, Teramoto S, et al. Outcome of patients with lung cancer detected via mass screening as compared to those presenting with symptoms. J Surg Oncol 1992; 50(1): 7-11. (IV)
- 15)Sobue T, Suzuki T, Matsuda M, et al. Survival for clinical stage I lung cancer not surgically treated. Comparison between screen-detected and symptom-detected cases. The Japanese Lung Cancer Screening Research Group. Cancer. 1992; 69(3): 685-92. (IV)
- 16)Satoh H, Ishikawa H, Yamashita YT, et al. Outcome of patients with lung cancer detected by mass screening versus presentation with symptoms. Anticancer Res. 1997; 17(3C): 2293-6. (IV)
- 17)Naruke T, Kuroishi T, Suzuki T, et al. Comparative study of survival of screen-detected compared with symptom-detected lung cancer cases. Japanese Lung Cancer Screening Research Group. Semin Surg Oncol. 1993; 9(2): 80-4. (IV)
- 18)Pretreatment evaluation of non-small-cell lung cancer. The American Thoracic Society and The European Respiratory Society. Am J Respir Crit Care Med. 1997; 156(1): 320-32. (IV)
1-2.検出方法
a.胸部X線写真
a.胸部X線写真
- 19)Quekel LG, Kessels AG, Goei R, et al. Miss rate of lung cancer on the chest radiograph in clinical practice. Chest. 1999; 115(3): 720-4. (V)
- 20)Soda H, Tomita H, Kohno S, et al. Limitation of annual screening chest radiography for the diagnosis of lung cancer. A retrospective study. Cancer. 1993; 72(8): 2341-6. (V)
- 21)Austin JH, Romney BM, Goldsmith LS. Missed bronchogenic carcinoma: radiographic findings in 27 patients with a potentially resectable lesion evident in retrospect. Radiology. 1992; 182(1): 115-22. (V)
- 22)Sone S, Li F, Yang ZG, et al. Characteristics of small lung cancers invisible on conventional chest radiography and detected by population based screening using spiral CT. Br J Radiol. 2000; 73(866): 137-45. (V)
- 23)Yang ZG, Sone S, Li F, et al. Visibility of small peripheral lung cancers on chest radiographs:influence of densitometric parameters, CT values and tumour type. Brit J Radiol. 2001; 74(877): 32-41. (V)
- 24)Quekel LG, Kessels AG, Goei R, et al. Detection of lung cancer on the chest radiograph: a study on observer performance. Eur J Radiol. 2001; 39(2): 111-6. (V)
b.胸部CT
- 25)Peuchot M, Libshitz HI. Pulmonary metastatic disease: radiologic-surgical correlation. Radiology. 1987; 164(3): 719-22. (V)
- 26)Altorki N, Kent M, Pasmantier M. Detection of early-stage lung cancer: Computed tomographic scan or chest radiograph? J Thorac Cardiovasc Surg. 2001; 121(6): 1053-7. (V)
- 27)Diederich S, Semik M, Lentschig MG, et al. Helical CT of pulmonary nodules in patients with extrathoracic malignancy: CT-surgical correlation. Am J Roentgenol. 1999; 172(2): 353-60. (V)
- 28)Kakinuma R, Ohmatsu H, Kaneko M, et al. Detection failures in spiral CT screening for lung cancer: analysis of CT findings. Radiology. 1999; 212(1): 61-6. (V)
- 29)Gurney JW. Missed lung cancer at CT: imaging findings in nine patients. Radiology. 1996; 199(1): 117-22. (V)
- 30)White CS, Romney BM, Mason AC, et al. Primary carcinoma of the lung overlooked at CT: analysis of findings in 14 patients. Radiology. 1996; 199(1): 109-15. (V)
- 31)Remy-Jardin M, Remy J, Giraud F, et al. Pulmonary nodules: detection with thick-section spiral CT versus conventional CT. Radiology. 1993; 187(2): 513-20. (V)
c.喀痰細胞診
- 32)MacDougall B, Weinerman B. The value of sputum cytology. J Gen Intern Med. 1992; 7(1): 11-3. (V)
- 33)Gledhill A, Bates C, Henderson D, et al. Sputum cytology: a limited role. J Clin Pathol. 1997; 50(7): 566-8. (V)
- 34)Sing A, Freudenberg N, Kortsik C, et al. Comparison of the sensitivity of sputum and brush cytology in the diagnosis of lung carcinomas. Acta Cytol. 1997; 41(2): 399-408. (V)
- 35)Bechtel JJ, Petty TL, Saccomanno G. Five year survival and later outcome of patients with X-ray occult lung cancer detected by sputum cytology. Lung Cancer. 2000; 30(1): 1-7. (V)
- 36)Frost JK, Ball WC Jr, Levin ML, et al. Early lung cancer detection: results of the initial (prevalence) radiologic and cytologic screening in the Johns Hopkins study. Am Rev Resp Dis. 1984; 130(4): 549-54. (II)
- 37)Melamed MR, Flehinger BJ, Zaman MB, et al. Screening for early lung cancer. Results of the Memorial Sloan-Kettering study in New York. Chest. 1984; 86(1): 44-53. (II)
- 38)Doria-Rose VP, Marcus PM, Szabo E, et al. Randomized controlled trials of the efficacy of lung cancer screening by sputum cytology revisited: a combined mortality analysis from the Johns Hopkins Lung Project and the Memorial Sloan-Kettering Lung Study. Cancer. 2009; 115(21): 5007-17. (II)
d.腫瘍マーカー,PET/CT
- 39)Bates SE. Clinical applications of serum tumor markers. Ann Intern Med. 1991; 115(8): 623-38. (IV)
- 40)Pujol JL, Boher JM, Grenier J, et al. Cyfra 21-1, neuron specific enolase and prognosis of non-small cell lung cancer: prospective study in 621 patients. Lung Cancer 2001; 31(2-3): 221-31. (V)
- 41)Maeda Y, Segawa Y, Takigawa N, et al. Clinical usefulness of serum cytokeratin 19 fragment as a tumor marker for lung cancer. Internal Med. 1996; 35(10): 764-71. (V)
- 42)Sugama Y, Kitamura S, Kawai T, et al. Clinical usefulness of CYFRA assay in diagnosing lung cancer: measurement of serum cytokeratin fragment. Jpn J Cancer Res. 1994; 85(11): 1178-84. (V)
- 43)Rastel D, Ramaioli A, Cornillie F, et al. CYFRA 21-1, a sensitive and specific new tumour marker for squamous cell lung cancer. Report of the first European multicentre evaluation. CYFRA 21-1 Multicentre Study Group. Eur J Cancer. 1994; 30A(5): 601-6. (V)
- 44)Pujol JL, Grenier J, Parrat E, et al. Cytokeratins as serum markers in lung cancer: a comparison of CYFRA 21-1 and TPS. Am J Respir Crit Care Med. 1996; 154(3 Pt 1): 725-33. (V)
- 45)Bombardieri E, Seregni E, Bogni A, et al. Evaluation of cytokeratin 19 serum fragments (CYFRA 21-1) in patients with lung cancer: results of a multicenter trial. Int J Biol Markers. 1994; 9(2): 89-95. (V)
- 46)Stieber P, Dienemann H, Schalhorn A, et al. Pro-gastrin-releasing peptide (ProGRP)--a useful marker in small cell lung carcinomas. Anticancer Res. 1999; 19(4A): 2673-8. (V)
- 47)Ebert W, Hoppe M, Muley T, et al. Monitoring of therapy in inoperable lung cancer patients by measurement of CYFRA 21-1, TPA- TP CEA, and NSE. Anticancer Res. 1997; 17(4B): 2875-8. (V)
- 48)Jørgensen LG, Osterlind K, Genollá J, et al. Serum neuron-specific enolase (S-NSE) and the prognosis in small-cell lung cancer (SCLC): a combined multivariable analysis on data from nine centres. Br J Cancer. 1996; 74(3): 463-7. (V)
- 49)Salgia R, Harpole D, Herndon JE 2nd, et al. Role of serum tumor markers CA 125 and CEA in non-small cell lung cancer. Anticancer Res. 2001; 21(2B): 1241-6. (V)
- 50)Satoh H, Ishikawa H, Kamma H, et al. Serum sialyl lewis X-i antigen levels in non-small cell lung cancer: correlation with distant metastasis and survival. Clin Cancer Res. 1997; 3(4): 495-9. (V)
- 51)Lindell RM, Hartman TE, Swensen SJ, et al. Lung cancer screening experience: a retrospective review of PET in 22 non-small cell lung carcinomas detected on screening chest CT in a high-risk population. AJR Am J Roentgenol. 2005; 185(1): 126-31. (IV)
- 52)Fortes DL, Allen MS, Lowe VJ, et al. The sensitivity of 18F-fluorodeoxyglucose positron emission tomography in the evaluation of metastatic pulmonary nodules. Eur J Cardiothorac Surg. 2008; 34(6): 1223-7. (IV)
- 53)Cronin P, Dwamena BA, Kelly AM, et al. Solitary pulmonary nodules and masses: a meta-analysis of the diagnostic utility of alternative imaging tests. Eur Radiol. 2008; 18(9): 1840-56. (I)
- 54)Cronin P, Dwamena BA, Kelly AM, et al. Solitary pulmonary nodules: meta-analytic comparison of cross-sectional imaging modalities for diagnosis of malignancy. Radiology. 2008; 246(3): 772-82. (I)
