
2
Ⅰ.肺癌の診断
確定診断
文献検索と採択
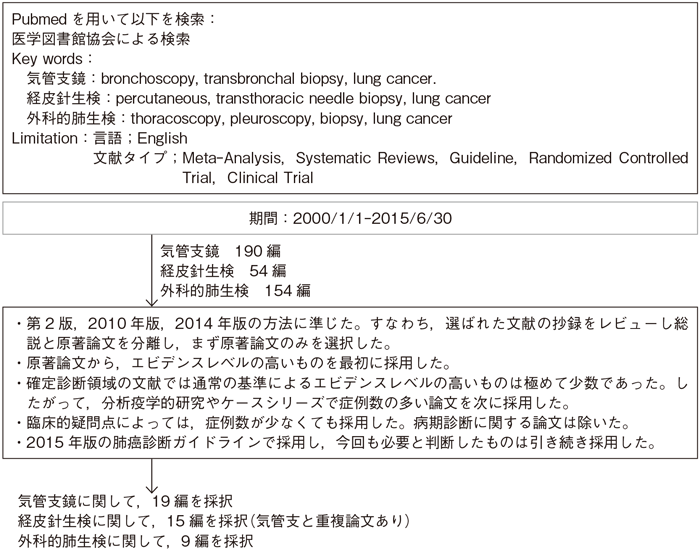
2-1.確定診断
- 推 奨
- 一部の手術例を除き,組織もしくは細胞診断は治療開始前に行うように勧められる。その方法としては,経気管支生検,経皮生検,胸腔鏡下生検,開胸生検などがあり,患者の状況と施設の状況から適切な方法を用いるべきである。(グレードA)
a.中枢気管支の病変を疑った場合に気管支鏡を施行するよう勧められる。(グレードA)
b.肺結節の確定診断については病変の大きさ,性状,部位などにより診断率が異なることを考慮のうえで,経気管支生検を施行するように勧められる。(グレードB)
c.経皮針生検は気管支鏡で診断困難な肺結節,縦隔病変の診断に有効であるが,空気塞栓,腫瘍細胞の播種,気胸などの合併症の可能性を考慮し,適応症例を選択したうえで行うことを考慮してもよい。(グレードC1)
d.胸腔鏡,開胸による生検は,気管支鏡や経皮針生検と比較して侵襲が大きいため,その必要性を十分に考慮したうえで行うことを考慮してもよい。(グレードC1)
エビデンス
- a・b.
- 中心型肺癌に対する気管支鏡の診断感度は88%で,鉗子生検の感度は74%,洗浄細胞診,ブラシ細胞診の感度は48%,59%と報告されている1)。中枢型肺癌に対して針吸引を行う際に,迅速細胞診を追加することにより診断率が向上することが報告されている2)。末梢型肺癌に対する気管支鏡の感度は78%で,鉗子生検の感度は57%,洗浄細胞診,ブラシ細胞診の感度は43%,54%と報告されている1)。診断感度は病変の大きさに依存し,2 cm以上の病変は63%,2 cm未満は34%と報告されている1)。
2010年に日本呼吸器内視鏡学会認定および関連施設で,すべての疾患に診断的に行われた気管支鏡件数は103,978件(うち,中枢気道病変24,283件,末梢孤立性病変60,275件)で,それぞれの合併症の頻度は1.32%(出血0.89%),1.55%(出血0.63%,気胸0.44%)であった3)。
近年,肺癌診断に以下の技術,手技が導入されている。自家蛍光気管支鏡は,白色光観察に併用すると,前浸潤性病変(扁平上皮異形成,上皮内癌)に対する検出感度が上昇すると報告され4)~8),メタアナリシスでは白色光単独の感度が43%に対して,自家蛍光併用の感度は85%,相対的感度は2.04倍である7)。一方,自家蛍光併用の特異度は,白色光単独に比べて低く,メタアナリシスではそれぞれ61%,80%と報告されている7)。同様の目的で狭域帯光観察気管支鏡が検討され,自家蛍光気管支鏡に比較して同等の感度で特異度は高いという報告がある9)。
気管支腔内超音波断層法(EBUS)に関しては,コンベックス型EBUS下の経気管支針生検(EBUS-TBNA)は主に,病期診断のために縦隔,肺門リンパ節に対して行われる(病期診断の章参照)。ラディアル型EBUS下の経気管支生検は末梢病変の診断に有用とされ1),小型病変に対する診断率の向上10)11),経気管支針生検(TBNA)の併用が有効であること12)が報告されている。一方,EBUSの経験の乏しい術者を含めた試験でガイドシース併用ラディアル型EBUSを使用しても感度が上昇しなかった報告もある13)。ラディアル型EBUS下の経気管支生検は,CTガイド下経皮針生検と比較すると,サイズ別では2 cm未満の病変に対する診断率は劣るが14),全体では有意差はなく,一方で合併症は有意に少ない14)15)。メタアナリシスではラディアル型EBUSの肺癌検出の感度は73%と報告されているが,対象集団の癌の割合,病変のサイズによって異なる16)。
肺末梢小型病変に対して診断率の向上を目的として,細径および極細径気管支鏡,仮想気管支鏡によるナビゲーションシステムが臨床に導入され,細径気管支鏡とラディアル型EBUSを組み合わせた手法において,ナビゲーションにより診断率が向上し,検査時間が短縮されることが報告された17)。極細径気管支鏡とX線透視を組み合わせた手法では,ナビゲーションはCTで肺野外層に存在する病変,右上葉の病変,X線写真で見えない病変に有効と報告された18)。これらの手法のメタアナリシスでは,ラディアル型EBUS,ガイドシース法,極細径気管支鏡,仮想気管支鏡ナビゲーションの診断率は71.1%,73.2%,70.0%,72.0%と報告されている19)。 - c.
- 従来,経皮吸引細胞診が行われ,その肺癌診断能はメタアナリシスでは感度86.1%,特異度98%と報告されていた20)。吸引細胞診では悪性病変の偽陰性率が高いため21),近年はCTガイド下に生検を行うことが多く,診断精度は,従来の経気管支生検と比較して高く1),特に直径2 cm以下の末梢病変の診断では優れていると報告されている14)。肺癌診断における感度は90%以上である1)22)。一方で,経皮針生検は,経気管支生検と比較して合併症が多いのが問題であるとされている1)14)15)。
近年ではground-glass nodule(GGN)に対しても経皮針生検が有用であるとする報告があり,メタアナリシスでは感度92%,特異度94%とされている23)~25)。このためGGNに長期にわたる経過観察を実施するのではなく積極的なCTガイド組織診による診断を推奨する報告もある25)。また使用する針は,Tru-cut-type針のほうが,modified Menghini-typeより診断率が高いと報告されている26)。
経皮針生検の主たる合併症は気胸と出血で,頻度は経皮針生検がラディアル型EBUS下の経気管支生検より高く15),気胸が16~52%,喀血をきたす出血が8~23%25)程度である。また頻度は少ないが,その他の重篤な合併症として空気塞栓(0.21~0.4%)27)28),胸膜播種(0.06~0.56%)27)29)~31)がある。 - d.
- 胸腔鏡による診断の良い適応となるのは胸膜に近い病変である32)。画像診断で悪性が強く疑われ,経気管支肺生検や経皮針生検による診断が困難な症例では胸腔鏡による診断を施行される場合もある33)。EBUSや胸腔鏡による生検が困難な縦隔リンパ節の生検にも適応がある34)35)。
胸腔鏡による診断は,ほぼ100%の感度,特異度をもつ。しかし全身麻酔が必要で侵襲が高く,手術による死亡率は0~0.5%,合併症の頻度は3~9.6%で,その内訳は,無気肺,肺炎,エアリークが含まれる36)。
通常,前処置は不要であるが,小結節や胸膜から遠い位置にある病変,淡い病変などは術前にマーキングが必要となる37)38)。気胸,出血などの合併症,マーカーの消失や脱落に留意する必要がある。また非常に稀であるが空気塞栓の報告例がある39)。
近年,胸水貯留例に診断と胸水ドレナージ,胸膜癒着術などの治療をかねて,胸腔鏡(medical thoracoscopy, pleuroscopy)が行われ,感度97.8%,特異度100%と報告されている40)。
引用文献
気管支鏡
- 1)Rivera MP, Mehta AC, Wahidi MM. Establishing the Diagnosis of Lung Cancer: Diagnosis and Management of Lung Cancer, 3rd ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2013; 143(5 Suppl): e142S-65S. (I)
- 2)Mondoni M, Carlucci P, Di Marco F, et al. Rapid on-site evaluation improves needle aspiration sensitivity in the diagnosis of central lung cancers: a randomized trial. Respiration. 2013; 86(1): 52-8. (II)
- 3)Asano F, Aoe M, Ohsaki Y, et al. Deaths and complications associated with respiratory endoscopy: a survey by the Japan Society for Respiratory Endoscopy in 2010. Respirology. 2012; 17(3): 478-85. (IV)
- 4)Häussinger K, Becker H, Stanzel F, et al. Autofluorescence bronchoscopy with white light bronchoscopy compared with white light bronchoscopy alone for the detection of precancerous lesions: a European randomised controlled multicentre trial. Thorax. 2005; 60(6): 496-503. (II)
- 5)Chen W, Gao X, Tian Q, et al. A comparison of autofluorescence bronchoscopy and white light bronchoscopy in detection of lung cancer and preneoplastic lesions: a meta-analysis. Lung Cancer. 2011; 73(2): 183-8. (I)
- 6)Wang Y, Wang Q, Feng J, et al. Comparison of autofluorescence imaging bronchoscopy and white light bronchoscopy for detection of lung cancers and precancerous lesions. Patient Prefer Adherence. 2013; 7: 621-31. (I)
- 7)Sun J, Garfield DH, Lam B, et al. The value of autofluorescence bronchoscopy combined with white light bronchoscopy compared with white light alone in the diagnosis of intraepithelial neoplasia and invasive lung cancer: a meta-analysis. J Thorac Oncol. 2011; (8): 1336-44. (I)
- 8)Wisnivesky JP, Yung RC, Mathur PN, et al. Diagnosis and treatment of bronchial intraepithelial neoplasia and early lung cancer of the central airways: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013; 143(5 Suppl): e263S-77S. (I)
- 9)Herth FJ, Eberhardt R, Anantham D, et al. Narrow-band imaging bronchoscopy increases the specificity of bronchoscopic early lung cancer detection. J Thorac Oncol. 2009; 4(9): 1060-5. (II)
- 10)Paone G, Nicastri E, Lucantoni G, et al. Endobronchial ultrasound-driven biopsy in the diagnosis of peripheral lung lesions. Chest. 2005; 128(5): 3551-7. (II)
- 11)Sánchez-Font A, Giralt L, Vollmer I, et al. Endobronchial ultrasound for the diagnosis of peripheral pulmonary lesions. A controlled study with fluoroscopy. Arch Bronconeumol. 2014; 50(5): 166-71. (II)
- 12)Chao TY, Chien MT, Lie CH, et al. Endobronchial ultrasonography-guided transbronchial needle aspiration increases the diagnostic yield of peripheral pulmonary lesions: a randomized trial. Chest. 2009; 136(1): 229-36. (II)
- 13)Roth K, Eagan TM, Andreassen AH, et al. A randomised trial of endobronchial ultrasound guided sampling in peripheral lung lesions. Lung Cancer. 2011; 74(2): 219-25. (II)
- 14)Fielding DI, Chia C, Nguyen P, et al. Prospective randomised trial of endobronchial ultrasound-guide sheath versus computed tomography-guided percutaneous core biopsies for peripheral lung lesions. Intern Med J. 2012; 42(8): 894-900. (II)
- 15)Steinfort DP, Vincent J, Heinze S, et al. Comparative effectiveness of radial probe endobronchial ultrasound versus CT-guided needle biopsy for evaluation of peripheral pulmonary lesions: a randomized pragmatic trial. Respir Med. 2011; 105(11): 1704-11. (II)
- 16)Steinfort DP, Khor YH, Manser RL, et al. Radial probe endobronchial ultrasound for the diagnosis of peripheral lung cancer: systematic review and meta-analysis. Eur Respir J. 2011; 37(4): 902-10. (I)
- 17)Ishida T, Asano F, Yamazaki K, et al. Virtual bronchoscopic navigation combined with endobronchial ultrasound to diagnose small peripheral pulmonary lesions: a randomised trial. Thorax. 2011; 66(12): 1072-7. (II)
- 18)Asano F, Shinagawa N, Ishida T, et al. Virtual bronchoscopic navigation combined with ultrathin bronchoscopy. A randomized clinical trial. Am J Respir Crit Care Med. 2013; 188(3): 327-33. (II)
- 19)Wang Memoli JS, Nietert PJ, Silvestri GA. Meta-analysis of guided bronchoscopy for the evaluation of the pulmonary nodule. Chest. 2012; 142(2): 385-93. (I)
経皮針生検
- 20)Lacasse Y, Wong E, Guyatt GH, et al. Transthoracic needle aspiration biopsy for the diagnosis of localised pulmonary lesions: a meta-analysis. Thorax. 1999; 54(10): 884-93. (I)
- 21)Choi SH, Chae EJ, Kim JE, et al. Percutaneous CT-guided aspiration and core biopsy of pulmonary nodules smaller than 1 cm: analysis of outcomes of 305 procedures from a tertiary referral center. AJR Am J Roentgenol. 2013; 201(5): 964-70. (IV)
- 22)Detterbeck FC, DeCamp MM Jr, Kohman LJ, et al; American College of Chest Physicians. Lung cancer. Invasive staging: the guidelines. Chest. 2003; 123(1 Suppl): 167S-175S. (I)
- 23)Yamauchi Y, Izumi Y, Nakatsuka S, et al. Diagnostic performance of percutaneous core needle lung biopsy under multi-CT fluoroscopic guidance for ground-glass opacity pulmonary lesions. Eur J Radiol. 2011; 79(2): e85-9. (IV)
- 24)Yamagami T, Yoshimatsu R, Miura H, et al. Diagnostic performance of percutaneous lung biopsy using automated biopsy needles under CT-fluoroscopic guidance for ground-glass opacity lesions. Br J Radiol 2013; 86(1022): 20120447. (IV)
- 25)Yang JS, Liu YM, Mao YM, et al. Meta-analysis of CT-guided transthoracic needle biopsy for the evaluation of the ground-glass opacity pulmonary lesions. Br J Radiol. 2014; 87(1042): 20140276. (I)
- 26)Tombesi P, Nielsen I, Tassinari D, et al. Transthoracic ultrasonography-guided core needle biopsy of pleural-based lung lesions: prospective randomized comparison between a Tru-cut-type needle and a modified Menghini-type needle. Ultraschall Med. 2009; 30(4): 390-5. (II)
- 27)Ibukuro K, Tanaka R, Takeguchi T, et al. Air embolism and needle track implantation complicating CT-guided percutaneous thoracic biopsy: single-institution experience. AJR Am J Roentgenol. 2009; 193(5): W430-6. (IV)
- 28)Hiraki T, Fujiwara H, Sakurai J, et al. Nonfatal systemic air embolism complicating percutaneous CT-guided transthoracic needle biopsy: four cases from a single institution. Chest. 2007; 132(2): 684-90. (V)
- 29)Kim JH, Kim YT, Lim HK, et al. Management for chest wall implantation of non-small cell lung cancer after fine-needle aspiration biopsy. Eur J Cardiothorac Surg. 2003; 23(5): 828-32. (V)
- 30)Robertson EG, Baxter G. Tumour seeding following percutaneous needle biopsy: the real story! Clin Radiol. Clin Radiol. 2011; 66(11): 1007-14. (VI)
- 31)Wu CC, Maher MM, Shepard JA. Complications of CT-guided percutaneous needle biopsy of the chest: prevention and management. AJR Am J Roentgenol. 2011; 196(6): W678-82. (IV)
外科的肺生検
- 32)Hazelrigg SR, Nunchuck SK, LoCicero J 3rd. Video Assisted Thoracic Surgery Study Group data. Ann Thorac Surg. 1993; 56(5): 1039-43; discussion 1043-4. (IV)
- 33)Voltolini L, Rapicetta C, Luzzi L, et al. Pattern of recurrence and survival of c-Ia NSCLC diagnosed by transpleural methods. J Cardiovasc Surg(Torino). 2008; 49(5): 697-702. (IV)
- 34)Krishna G, Gould MK. Minimally invasive techniques for the diagnosis of peripheral pulmonary nodules. Curr Opin Pulm Med. 2008; 14(4): 282-6. (IV)
- 35)De Leyn P, Dooms C, Kuzdzal J, et al. Revised ESTS guidelines for preoperative mediastinal lymph node staging for non-small-cell lung cancer. Eur J Cardiothorac Surg. 2014; 45(5): 787-98. (I)
- 36)Jiménez MF. Prospective study on video-assisted thoracoscopic surgery in the resection of pulmonary nodules: 209 cases from the Spanish Video-Assisted Thoracic Surgery Study Group. Eur J Cardiothorac Surg. 2001; 19(5): 562-5. (III)
- 37)Khereba M, Ferraro P, Duranceau A, et al. Thoracoscopic localization of intraparenchymal pulmonary nodules using direct intracavitary thoracoscopic ultrasonography prevents conversion of VATS procedures to thoracotomy in selected patients. J Thorac Cardiovasc Surg. 2012; 144(5): 1160-5. (IV)
- 38)Gonfiotti A, Davini F, Vaggelli L, et al. Thoracoscopic localization techniques for patients with solitary pulmonary nodule: hookwire versus radio-guided surgery. Eur J Cardiothorac Surg. 2007; 32(6): 843-7. (II)
- 39)Sato K, Miyauchi K, Shikata F, et al. Arterial air embolism during percutaneous pulmonary marking under computed tomography guidance. Jpn J Thorac Cardiovasc Surg. 2005; 53(7): 404-6. (V)
- 40)Dhooria S, Singh N, Aggarwal AN, et al. A randomized trial comparing the diagnostic yield of rigid and semirigid thoracoscopy in undiagnosed pleural effusions. Respir Care. 2014; 59(5): 756-64. (II)
