
5
Ⅰ.肺癌の診断
病期診断
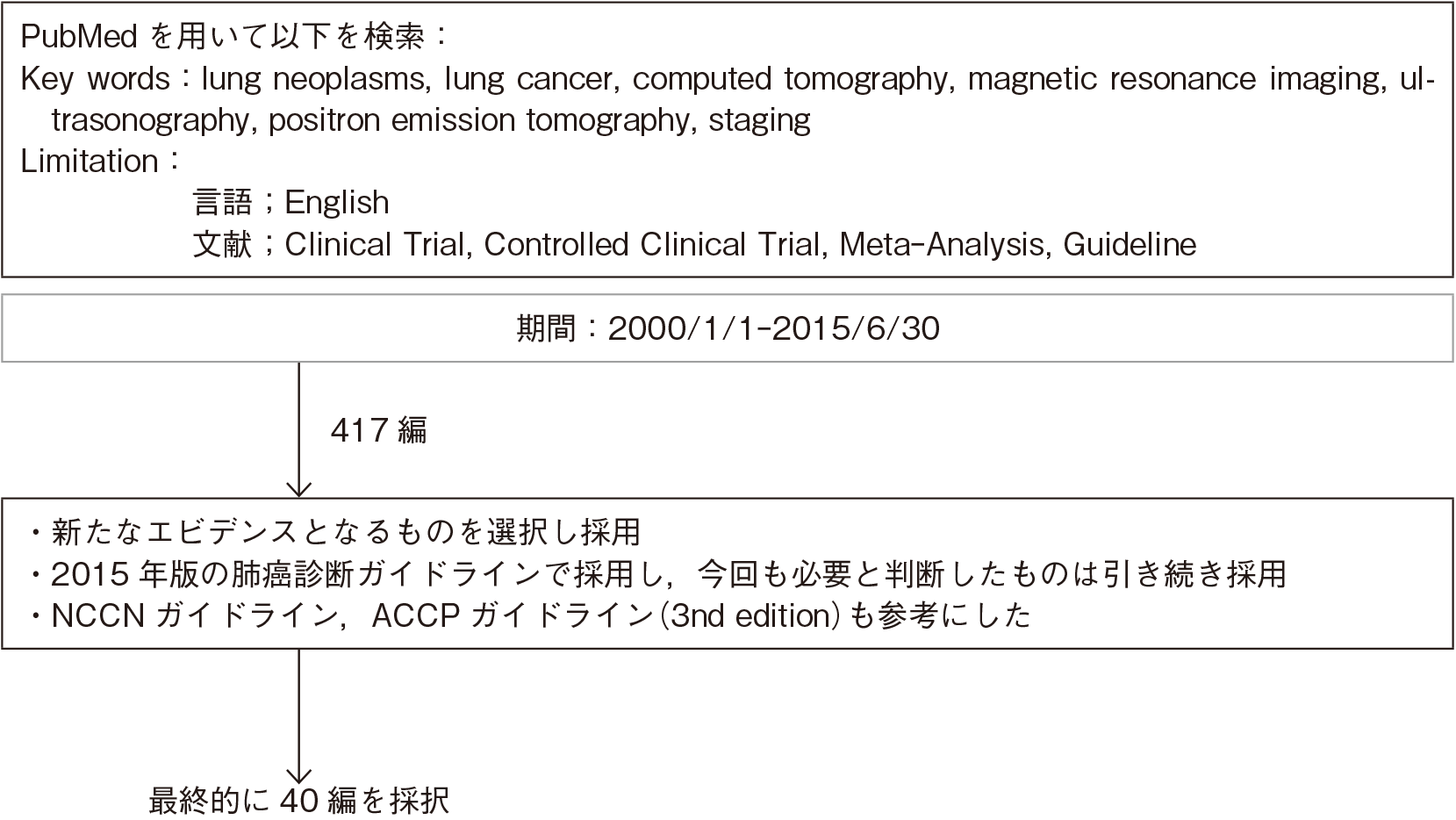
文献検索と採択
5-1.病期診断
- 推 奨
a.肺癌の治療方針の決定のために病期診断は必須で行うよう勧められる。(グレードA)
b.病期診断のために,胸部造影CTを行うよう勧められる。(グレードA)
c.原発巣が2 cm以下のGGNでconsolidationの比率が25%以下の症例を除き,病期診断のために,FDG-PET/CT,頭部造影MRIもしくはCTを行うよう勧められる。(グレードA)
d.FDG-PET/CTが施行し得ない場合は,上腹部まで(肝,副腎を完全に含む)の造影CTと骨シンチグラフィを施行するよう勧められる。(グレードB)
e.縦隔・肺門リンパ節転移の有無により治療法を選択する際,胸部造影CTでリンパ節腫大があるかFDG-PET/CTでFDG集積を認める所見を有する場合は,可能なかぎりEBUS-TBNA/EUS-FNAなどにより,病理学的な診断を得ることが勧められる。(グレードB)
f.FDG-PET/CTで,単発の遠隔転移が疑われた場合は,可能なかぎり他の画像診断や病理学的診断で転移であることを確認することが勧められる。(グレードB)
エビデンス
- a.
- 肺癌のTNM分類による病期診断により予後予測が可能で1),病期分類に従った治療方針決定のために必須である。
- b・c.
- CTでは病変の存在,大きさ,広がり,正常構造との関係を正確に捉えることができ,また無気肺や閉塞性肺炎の有無,隣接臓器への浸潤の診断にも有用であり,病期診断において侵襲的検査の前に最初に行うべき基本検査である。
原発巣の診断において,FDG-PET単独では十分な情報が得られないことがある。CTによる解剖学的情報と統合したFDG-PET/CTでは,縦隔浸潤,胸壁浸潤,腫瘍周囲の無気肺との鑑別に有用2)で,T因子の正診率が82%であり,FDG-PET単独の55%,CT単独の68%と比べて高い3)。遠隔転移の検索において,FDG-PET/CTは造影CTに比べ感度・特異度が高く,FDG-PET/CTによる遠隔転移診断の感度が77~100%,特異度が93~100%との報告や4)~7),肝,副腎での陰性的中率が95%,骨では90%との報告がある8)9)。
脳転移の検索において,造影MRIは造影CTや単純CT,MRIに比べて,高い感度を示し,腫瘍径の小さな転移を多く検出すると報告されている10)11)が,体内金属などにより造影MRI撮影ができない場合は,造影CTでも代用可能である。脳転移検索におけるFDG-PET/CTについては18FDGは正常脳組織への集積がみられるために感度は24~27%12)13)と低く勧められない。
原発巣が2 cm以下のGGN(ground-glass nodule)でconsolidationの比率が25%以下の症例は遠隔転移がほとんどないことが報告されており14),このような症例は確定診断を待たずに手術を施行する症例も多く,FDG-PET/CT,頭部造影MRIもしくはCTなどによる病期診断は必須ではない。 - d.
- コントロール不良の糖尿病,閉所恐怖症,自施設および近隣の施設にPET/CTの設備がないなど,FDG-PET/CTが施行し得ない場合,造影CTはFDG-PET/CTに比べると転移巣検索の感度・特異度は劣るものの,転移巣は原則として血流が豊富で造影CTでの造影効果が高いため,肝,副腎,腎などへの転移検索に造影CTは有用である15)。
また,骨転移の検索に関して,複数のメタアナリシスで骨シンチグラフィの感度82~86%,特異度62~88%と報告されており16)17),FDG-PET/CTの感度92%,特異度98%に比べるとやや劣るものの,Schirrmeisterらの報告では無症候の肺癌患者に骨シンチグラフィを施行しなかった場合,14~22%の患者が骨転移を見逃されるとされ18),FDG-PET/CTが施行し得ない場合には骨シンチグラフィを施行するように勧められる。しかし,外傷や変形性関節症などでは偽陽性となり得るため注意が必要である。 - e.
- N因子の診断はCT・MRIでは,短径が1 cm以上のリンパ節腫大を転移陽性と診断する基準が用いられる19)20)が,この大きさによる診断基準を用いたCTの成績は,感度52~75%,特異度66~88%であり21)~24),診断能は高くない。一方,Billéらの報告でFDG-PET/CTの縦隔リンパ節の診断能は感度54.2%,特異度91.9%,陽性的中率74.3%,陰性的中率82.3%,正診率80.5%で25),最近のメタアナリシスでFDG-PET/CT縦隔リンパ節の診断能は,感度71~85%,特異度85~91%とCT,MRIに比較して明らかに高い診断能を示す7)16)26)27)。したがって,手術適応と考えられる症例で,縦隔リンパ節評価にFDG-PET/CTは勧められる。しかし,感染性疾患や肉芽腫性疾患において,FDG-PET/CTによる縦隔リンパ節の偽陽性率が高くなることも指摘されており27),特に結核などの肉芽腫性疾患が比較的多い本邦では注意が必要である。
EBUS-TBNAの合併症頻度は1.23%でその多くは軽度の出血や感染で,縦隔鏡や胸腔鏡に比べて低侵襲で検体採取が可能な検査であり28),高齢者でも合併症に差はないとの報告がある29)。肺癌の縦隔リンパ節転移診断におけるEBUS-TBNAの有用性をみたメタアナリシスでは,感度90~93%,特異度99~100%で30)31),画像上縦隔リンパ節腫大がある患者とない患者でのサブグループ解析による感度はそれぞれ94%と76%で,両群間に有意差があると報告されている30)。また同様にEUS-FNAの有用性をみたメタアナリシスでは,画像上縦隔リンパ節腫大がある患者の感度90%,特異度97%に対し,画像上縦隔リンパ節腫大のない患者では感度58%,特異度98%と報告されており32),胸部造影CTで腫大があるかFDG-PET/CTでFDG集積のある縦隔・肺門リンパ節に関しては,可能なかぎりEBUS-TBNA/EUS-FNAなどにより病理学的な診断を得ることが勧められる33)が,画像上縦隔リンパ節転移の疑われない症例も含めた全例に施行する意義は少ないと考えられる。また,EBUS-TBNAとEUS-FNAを併用することで縦隔リンパ節転移診断の感度・特異度ともに向上することが示されており34),両者の併用を考慮してもよい。 - f.
- 遠隔転移の検索にFDG-PET/CTは有用であるが,感染性疾患,肉芽腫性疾患,副腎腺腫などで偽陽性となることが指摘されている27)35)。
特に副腎は肺癌の転移先として最も多い臓器の1つであり36),副腎腺腫との鑑別は重要である。CTで一側性の副腎腫大がみられた場合に副腎転移の可能性が高いとする報告もあるが4),有意でないとの報告もあり37),それだけで良悪性の判断はできない。MRIの脂肪抑制画像やdynamic MRIなどの検査を組み合わせたり,経皮針生検などが有用であることが指摘されており38)~40),単発の遠隔転移が疑われた場合は,可能なかぎり他の画像診断や病理学的診断で転移であることを確認することが勧められる。
引用文献
- 1)Goldstraw P, Crowley J, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming(seventh)edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007; 2(8): 706-14. (IV)
- 2)Steinert HC. PET and PET-CT of lung cancer. Methods Mol Biol. 2011; 727: 33-51. (IV)
- 3)De Wever W, Stroobants S, Coolen J, et al. Integrated PET/CT in the staging of nonsmall cell lung cancer: technical aspects and clinical integration. Eur Respir J. 2009; 33(1): 201-12. (IV)
- 4)Antoch G, Stattaus J, Nemat AT, et al. Non-small cell lung cancer: dual-modality PET/CT in preoperative staging. Radiology. 2003; 229(2): 526-33. (IV)
- 5)Cerfolio RJ, Ojha B, Bryant AS, et al. The accuracy of integrated PET-CT compared with dedicated PET alone for the staging of patients with nonsmall cell lung cancer. Ann Thorac Surg. 2004; 78(3): 1017-23. (III)
- 6)De Wever W, Ceyssens S, Mortelmans L, et al. Additional value of PET-CT in the staging of lung cancer: comparison with CT alone, PET alone and visual correlation of PET and CT. Eur Radiol. 2007; 17(1): 23-32. (IV)
- 7)Wu Y, Li P, Zhang H, et al. Diagnostic value of fluorine 18 fluorodeoxyglucose positron emission tomography/computed tomography for the detection of metastases in non-small-cell lung cancer patients. Int J Cancer. 2013; 132(2): E37-47. (I)
- 8)Silvestri GA, Littenberg B, Colice GL. The clinical evaluation for detecting metastatic lung cancer. A meta-analysis. Am J Respir Crit Care Med. 1995; 152(1): 225-30. (I)
- 9)Silvestri GA, Tanoue LT, Margolis ML, et al. The noninvasive staging of non-small cell lung cancer: the guidelines. Chest. 2003; 123(1 Suppl): 147S-156S. (IV)
- 10)Davis PC, Hudgins PA, Peterman SB, et al. Diagnosis of cerebral metastases: double-dose delayed CT vs contrast-enhanced MR imaging. AJNR Am J Neuroradiol. 1991; 12(2): 293-300. (IV)
- 11)Akeson P, Larsson EM, Kristoffersen DT, et al. Brain metastases--comparison of gadodiamide injection-enhanced MR imaging at standard and high dose, contrast-enhanced CT and non-contrast-enhanced MR imaging. Acta Radiol. 1995; 36(3): 300-6. (III)
- 12)Krüger S, Mottaghy FM, Buck AK, et al. Brain metastasis in lung cancer. Comparison of cerebral MRI and 18F-FDG-PET/CT for diagnosis in the initial staging. Nuklearmedizin. 2011; 50(3): 101-6. (III)
- 13)Lee HY, Lee KS, Kim BT, et al. Diagnostic efficacy of PET/CT plus brain MR imaging for detection of extrathoracic metastases in patients with lung adenocarcinoma. J Korean Med Sci. 2009; 24(6): 1132-8. (III)
- 14)Suzuki K, Koike T, Asakawa T, et al. A prospective radiological study of thin-section computed tomography to predict pathological noninvasiveness in peripheral clinical IA lung cancer(Japan Clinical Oncology Group 0201). J Thorac Oncol. 2011; 6(4): 751-6. (IV)
- 15)Pretreatment evaluation of non-small-cell lung cancer. The American Thoracic Society and The European Respiratory Society. Am J Respir Crit Care Med. 1997; 156(1): 320-32. (IV)
- 16)Silvestri GA, Gould MK, Margolis ML, et al. Noninvasive staging of non-small cell lung cancer: ACCP evidenced-based clinical practice guidelines(2nd edition). Chest. 2007; 132(3 Suppl): 178S-201S. (IV)
- 17)Qu X, Huang X, Yan W, et al. A meta-analysis of 18FDG-PET-CT, 18FDG-PET, MRI and bone scintigraphy for diagnosis of bone metastases in patients with lung cancer. Eur J Radiol. 2012; 81(5): 1007-15. (I)
- 18)Schirrmeister H, Arslandemir C, Glatting G, et al. Omission of bone scanning according to staging guidelines leads to futile therapy in non-small cell lung cancer. Eur J Nucl Med Mol Imaging. 2004; 31(7): 964-8. (III)
- 19)Glazer GM, Gross BH, Quint LE, et al. Normal mediastinal lymph nodes: number and size according to American Thoracic Society mapping. AJR Am J Roentgenol. 1985; 144(2): 261-5. (III)
- 20)Kiyono K, Sone S, Sakai F, et al. The number and size of normal mediastinal lymph nodes: a postmortem study. AJR Am J Roentgenol. 1988; 150(4): 771-6. (IV)
- 21)McLoud TC, Bourgouin PM, Greenberg RW, et al. Bronchogenic carcinoma: analysis of staging in the mediastinum with CT by correlative lymph node mapping and sampling. Radiology. 1992; 182(2): 319-23. (IV)
- 22)Birim O, Kappetein AP, Stijnen T, et al. Meta-analysis of positron emission tomographic and computed tomographic imaging in detecting mediastinal lymph node metastases in nonsmall cell lung cancer. Ann Thorac Surg. 2005; 79(1): 375-82. (I)
- 23)van Tinteren H, Hoekstra OS, Smit EF, et al. Effectiveness of positron emission tomography in the preoperative assessment of patients with suspected non-small-cell lung cancer: the PLUS multicentre randomised trial. Lancet. 2002; 359(9315): 1388-93. (II)
- 24)Dales RE, Stark RM, Raman S. Computed tomography to stage lung cancer. Approaching a controversy using meta-analysis. Am Rev Respir Dis. 1990; 141(5 Pt 1): 1096-101. (I)
- 25)Billé A, Pelosi E, Skanjeti A, et al. Preoperative intrathoracic lymph node staging in patients with non-small-cell lung cancer: accuracy of integrated positron emission tomography and computed tomography. Eur J Cardiothorac Surg. 2009; 36(3): 440-5. (IV)
- 26)Gould MK, Kuschner WG, Rydzak CE, et al. Test performance of positron emission tomography and computed tomography for mediastinal staging in patients with non-small-cell lung cancer: a meta-analysis. Ann Intern Med. 2003; 139(11): 879-92. (I)
- 27)Paul NS, Ley S, Metser U. Optimal imaging protocols for lung cancer staging: CT, PET, MR imaging, and the role of imaging. Radiol Clin North Am. 2012; 50(5): 935-49. (IV)
- 28)Asano F, Aoe M, Ohsaki Y, et al. Complications associated with endobronchial ultrasound-guided transbronchial needle aspiration: a nationwide survey by the Japan Society for Respiratory Endoscopy. Respir Res. 2013; 14: 50. (IV)
- 29)Evison M, Crosbie PA, Martin J, et al. EBUS-TBNA in elderly patients with lung cancer: safety and performance outcomes. J Thorac Oncol. 2014; 9(3): 370-6. (IV)
- 30)Gu P, Zhao YZ, Jiang LY, et al. Endobronchial ultrasound-guided transbronchial needle aspiration for staging of lung cancer: a systematic review and meta-analysis. Eur J Cancer. 2009; 45(8): 1389-96. (I)
- 31)Dong X, Qiu X, Liu Q, et al. Endobronchial ultrasound-guided transbronchial needle aspiration in the mediastinal staging of non-small cell lung cancer: a meta-analysis. Ann Thorac Surg. 2013; 96(4): 1502-7. (I)
- 32)Micames CG, McCrory DC, Pavey DA, et al. Endoscopic ultrasound-guided fine-needle aspiration for non-small cell lung cancer staging: A systematic review and metaanalysis. Chest. 2007; 131(2): 539-48. (I)
- 33)Tournoy KG, Maddens S, Gosselin R, et al. Integrated FDG-PET/CT does not make invasive staging of the intrathoracic lymph nodes in non-small cell lung cancer redundant: a prospective study. Thorax. 2007; 62(8): 696-701. (III)
- 34)Zhang R, Ying K, Shi L, et al. Combined endobronchial and endoscopic ultrasound-guided fine needle aspiration for mediastinal lymph node staging of lung cancer: a meta-analysis. Eur J Cancer. 2013; 49(8): 1860-7. (I)
- 35)Pieterman RM, van Putten JW, Meuzelaar JJ, et al. Preoperative staging of non-small-cell lung cancer with positron-emission tomography. N Engl J Med. 2000; 343(4): 254-61. (IV)
- 36)Carr LL, Finigan JH, Kern JA. Evaluation and treatment of patients with non-small cell lung cancer. Med Clin North Am. 2011; 95(6): 1041-54. (IV)
- 37)Oliver TW Jr, Bernardino ME, Miller JI, et al. Isolated adrenal masses in nonsmall-cell bronchogenic carcinoma. Radiology. 1984; 153(1): 217-8. (IV)
- 38)Heinz-Peer G, Hönigschnabl S, Schneider B, et al. Characterization of adrenal masses using MR imaging with histopathologic correlation. AJR Am J Roentgenol. 1999; 173(1): 15-22. (IV)
- 39)Gillams A, Roberts CM, Shaw P, et al. The value of CT scanning and percutaneous fine needle aspiration of adrenal masses in biopsy-proven lung cancer. Clin Radiol. 1992; 46(1): 18-22. (IV)
- 40)Chong S, Lee KS, Kim HY, et al. Integrated PET-CT for the characterization of adrenal gland lesions in cancer patients: diagnostic efficacy and interpretation pitfalls. Radiographics. 2006; 26(6): 1811-24. (IV)
