
4
Ⅲ.小細胞肺癌
再発小細胞肺癌
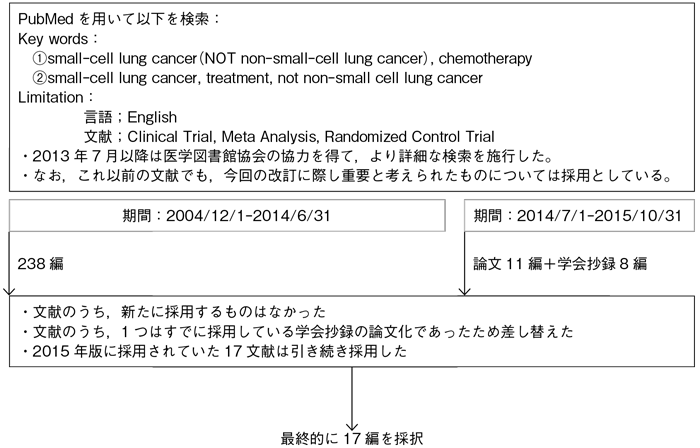
文献検索と採択
本文中に用いた略語および用語の解説
| AMR | アムルビシン | |
|---|---|---|
| CDDP | シスプラチン | |
| CPT-11 | イリノテカン | |
| ETP | エトポシド | |
| NGT | ノギテカン | |
| BSC | best supportive care | 緩和治療 |
| G-CSF | granulocyte colony stimulating factor | 顆粒球刺激因子 |
| MST | median survival time | 生存期間中央値 |
| OS | overall survival | 全生存期間 |
| SCLC | small cell lung cancer | 小細胞肺癌 |
再発小細胞肺癌におけるSensitive relapseとRefractory relapseの分類について
樹形図
4-1.再発小細胞肺癌に対する化学療法
- 推 奨
a.Sensitive relapseには,化学療法を行うよう推奨される。(グレードA)
b.Refractory relapseには,標準治療は確立していないが,全身状態を考慮したうえで,化学療法を行うよう推奨される。(グレードC1)
エビデンス
- a.
- 初回治療終了後45日以上経過して再発を認めたSensitive relapseでは,BSCと比較してNGTでOSの有意な延長が報告されており6),Sensitive relapseに対しては化学療法を行うことが推奨される。
Sensitive relapseに対して,これまで複数の第Ⅲ相試験が報告されている6)~11)。このうち4つの比較試験では,いずれもNGTの有効性が報告されているため,現時点ではNGTがSensitive relapseに対する標準治療とみなされているが,各臨床試験の症例数が少なく,確立したものではない。しかし,本邦で行われたJCOG0605では,NGTに対するCDDP+ETP+CPT-11併用療法の優越性が比較第Ⅲ相試験で証明された(MSTで18.2カ月vs 12.5カ月)。よって,患者の条件が許せば同併用療法はオプションの1つとなり得る11)。
Sensitive relapseに対する複数の比較試験や第Ⅱ相試験により,ETP2),CPT-1112),AMR10)13)14)の有効性が報告されているが,いずれも第Ⅲ相試験で有効性が確認されておらず,標準治療とはみなされていない。
比較的全身状態が保たれたSensitive relapse患者に対して,初回化学療法と同じレジメンを再投与すること(re-challenge)の有効性も報告されているが15)16),1980年代の古い報告であり,これ以後re-challengeの有効性を前向きに検討した報告はなく,その意義は確立していない。 - b.
- Refractory relapseに対する化学療法の意義は確立していない。しかし,再発小細胞肺癌に対するNGTとAMRの第Ⅲ相試験のサブグループ解析では,Refractory relapseにおいて,MSTがAMR 6.2カ月vs NGT 5.7カ月(P=0.0469)と,AMRにより生存期間の有意な延長を認めている10)。また,本邦においてもRefractory relapse症例に対するAMRの第Ⅱ相試験が行われ,奏効率は32.9%,MSTは8.9カ月であった17)。全身状態が良好な患者では,AMRを含む単剤の化学療法の実施を検討すべきである。
引用文献
- 1)Batist G, Carney DN, Cowan KH, et al. Etoposide(VP-16)and cisplatin in previously treated small-cell lung cancer: clinical trial and in vitro correlates. J Clin Oncol. 1986; 4(6): 982-6. (IV)
- 2)Johnson DH, Greco FA, Strupp J, et al. Prolonged administration of oral etoposide in patients with relapsed or refractory small-cell lung cancer: a phase II trial. J Clin Oncol. 1990; 8(10): 1613-7. (IV)
- 3)Giaccone G, Donadio M, Bonardi G, et al. Teniposide in the treatment of small-cell lung cancer: the influence of prior chemotherapy. J Clin Oncol. 1988; 6(8): 1264-70. (IV)
- 4)Ardizzoni A, Hansen H, Dombernowsky P, et al. Topotecan, a new active drug in the second-line treatment of small-cell lung cancer: a phase II study in patients with refractory and sensitive disease. The European Organization for Research and Treatment of Cancer Early Clinical Studies Group and New Drug Development Office, and the Lung Cancer Cooperative Group. J Clin Oncol. 1997; 15(5): 2090-6. (IV)
- 5)Kim YH, Goto K, Yoh K, et al. Performance status and sensitivity to first-line chemotherapy are significant prognostic factors in patients with recurrent small cell lung cancer receiving second-line chemotherapy. Cancer. 2008; 113(9): 2518-23. (IV)
- 6)O’Brien ME, Ciuleanu TE, Tsekov H, et al. Phase III trial comparing supportive care alone with supportive care with oral topotecan in patients with relapsed small-cell lung cancer. J Clin Oncol. 2006; 24(34): 5441-7. (II)
- 7)von Pawel J, Schiller JH, Shepherd FA, et al. Topotecan versus cyclophosphamide, doxorubicin, and vincristine for the treatment of recurrent small-cell lung cancer. J Clin Oncol. 1999; 17(2): 658-67. (II)
- 8)Eckardt JR, von Pawel J, Pujol JL, et al. Phase III study of oral compared with intravenous topotecan as second-line therapy in small-cell lung cancer. J Clin Oncol. 2007; 25(15): 2086-92. (II)
- 9)O’Bryan RM, Crowley JJ, Kim PN, et al. Comparison of etoposide and cisplatin with bis-chloro-ethylnitrosourea, thiotepa, vincristine, and cyclophosphamide for salvage treatment in small cell lung cancer. A Southwest Oncology Group Study. Cancer. 1990; 65(4): 856-60. (II)
- 10)von Pawel J, Jotte R, Spigel DR, et al. Randomized phase III trial of amrubicin versus topotecan as second-line treatment for patients with small-cell lung cancer. J Clin Oncol. 2014; 32(35): 4012-9. (II)
- 11)Goto K, Ohe Y, Seto T, et al. A randomized phase III study of cisplatin(CDDP), etoposide(ETOP)and irinotecan versus topotecan as second-line chemotherapy in patients with sensitive relapsed small-cell lung cancer(SCLC): Japan Clinical Oncology Group study JCOG0605. J Clin Oncol. 2014; 32: suppl; abstr7504. (II)
- 12)Masuda N, Fukuoka M, Kusunoki Y, et al. CPT-11: a new derivative of camptothecin for the treatment of refractory or relapsed small-cell lung cancer. J Clin Oncol. 1992; 10(8): 1225-9. (IV)
- 13)Inoue A, Sugawara S, Yamazaki K, et al. Randomized phase II trial comparing amrubicin with topotecan in patients with previously treated small-cell lung cancer: North Japan Lung Cancer Study Group Trial 0402. J Clin Oncol. 2008; 26(33): 5401-6. (II)
- 14)Jotte R, Conkling P, Reynolds C, et al. Randomized phase II trial of single-agent amrubicin or topotecan as second-line treatment in patients with small-cell lung cancer sensitive to first-line platinum-based chemotherapy. J Clin Oncol. 2011; 29(3): 287-93. (II)
- 15)Postmus PE, Berendsen HH, van Zandwijk N, et al. Retreatment with the induction regimen in small cell lung cancer relapsing after an initial response to short term chemotherapy. Eur J Cancer Clin Oncol. 1987; 23(9): 1409-11. (IV)
- 16)Giaccone G, Ferrati P, Donadio M, et al. Reinduction chemotherapy in small cell lung cancer. Eur J Cancer Clin Oncol. 1987; 23(11): 1697-9. (IV)
- 17)Murakami H, Yamamoto N, Shibata T, et al. A single-arm confirmatory study of amrubicin therapy in patients with refractory small-cell lung cancer: Japan Clinical Oncology Group Study(JCOG0901). Lung Cancer. 2014; 84(1): 67-72. (IV)
レジメン:再発小細胞肺癌
| AMR療法 | AMR | 40 mg/m2, day 1, 2, 3 | q3w |
|---|---|---|---|
| NGT療法 | NGT | 1.0 mg/m2, day 1, 2, 3, 4, 5 | q3w |
| CDDP+ETP+CPT-11療法 (G-CSF製剤予防投与有) |
CDDP | 25 mg/m2, day 1, weekly for 10 weeks | |
| ETP | 60 mg/m2, day 1, 2, 3, on weeks 1, 3, 5, 7, 9 | ||
| CPT-11 | 90 mg/m2, day 1, on weeks 2, 4, 6, 8, 10 | ||
