
4
Ⅰ.診 断
質的画像診断
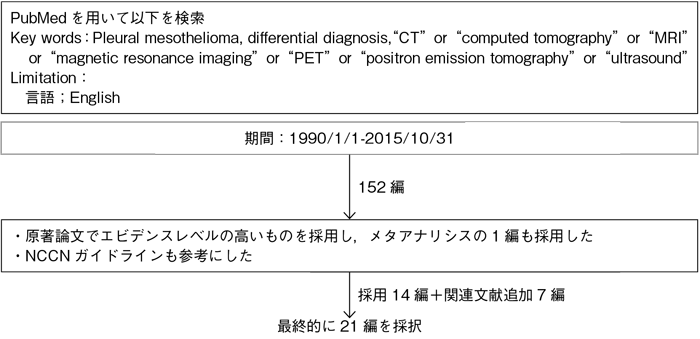
文献検索と採択
4-1.質的画像診断
- 推 奨
a.胸部造影CTは,胸膜病変の存在診断だけでなく,良悪性の鑑別に有用な情報が得られるため,行うよう勧められる。(グレードA)
b.FDG-PET/CTは,胸膜病変の良悪性鑑別の補助診断として行うことを考慮してもよい。(グレードC1)
エビデンス
胸膜中皮腫における頻度の高い画像所見として,胸水貯留,胸膜肥厚,患側胸郭の容積減少,局所浸潤,リンパ節腫大,転移が挙げられる。個々の所見は胸膜中皮腫の診断において非特異的であるが,これらの複数の所見は胸膜中皮腫の可能性を示唆するものであり,特に石綿曝露歴のある患者では胸膜中皮腫を積極的に疑う必要がある。
胸膜中皮腫の存在診断のために最初に施行される検査は,胸部単純X線撮影である1)。片側性胸水や,びまん性胸膜肥厚ないし胸膜腫瘤が比較的高頻度にみられる所見である。さらに,進行例では,患側胸郭の容積減少やリンパ節腫大が認められる。しかし,胸水貯留のみやわずかな胸膜肥厚がある早期の症例や,高度の胸膜プラークがみられる症例では,胸部単純X線写真による胸膜中皮腫の存在診断は困難である。
胸膜中皮腫の存在診断のために最初に施行される検査は,胸部単純X線撮影である1)。片側性胸水や,びまん性胸膜肥厚ないし胸膜腫瘤が比較的高頻度にみられる所見である。さらに,進行例では,患側胸郭の容積減少やリンパ節腫大が認められる。しかし,胸水貯留のみやわずかな胸膜肥厚がある早期の症例や,高度の胸膜プラークがみられる症例では,胸部単純X線写真による胸膜中皮腫の存在診断は困難である。
- a.
- 胸部造影CTは,胸膜中皮腫の存在診断において有用であり,胸膜肥厚と胸水貯留が高頻度に認められる所見である2)3)。CTは,胸膜病変の良悪性の鑑別にも有効である。①肺を取り囲む全周性の胸膜肥厚(pleural rind),②縦隔胸膜浸潤,③厚さが1 cmを越える胸膜肥厚,④結節状の胸膜肥厚,の4つの所見が重要であり,これらの一つないし複数の所見がある場合,悪性病変である可能性が極めて高い4)~6)。胸膜中皮腫と転移性胸膜腫瘍の鑑別に多変量解析が行われ,前述の①~③が有用との報告があるが6),両者の所見にはオーバーラップがかなりみられ鑑別は困難と考えられる。
MRIについては,CTにおける前述の4つの画像所見に,病変の信号強度7)8)や造影剤を用いたT1強調画像の所見9)10)を加えることが,胸膜病変の良悪性の鑑別に有用であるとする報告がある。また,拡散強調画像が胸膜病変の良悪性の鑑別に有用で,造影ダイナミック検査を追加するとさらに診断能が上昇するとする報告もある11)。 - b.
- 胸膜病変の良悪性の鑑別をグルコース代謝の多寡によって判定しようとするFDG-PETは,多くの研究によってその有用性が報告されている12)~15)。多時相で,定量評価として用いられているstandardized uptake value(SUV)を計測する方法(Dual time point FDG-PET)に関しては,悪性病変では遅延相での集積の増加が認められた14)15)。機能画像と形態画像の融合画像であるPET/CTでは,FDG-PET同様,良悪性の鑑別を行い良好な成績が報告されている16)~20)。多時相でSUV測定を行う方法(Dual time point PET/CT)の有用性も報告されている19)20)。しかし,胸膜病変の良悪性の鑑別におけるFDG-PETないしPET/CTに関するバイアスの少ない14論文のメタアナリシスでは,半定量的評価によるPET/CTの診断能は中等度(感度81%,特異度74%,Az値0.838)であり,鑑別のためのルーチンの検査として推奨できないと報告されており21),病期診断や遠隔転移の診断を含めて検査の適応を考慮する必要がある。
引用論文
- 1)Nickell LT Jr, Lichtenberger JP 3rd, Khorashadi L, et al. Multimodality imaging for characterization, classification, and staging of malignant pleural mesothelioma. Radiographics. 2014; 34(6): 1692-706. (IV)
- 2)Kawashima A, Libshitz HI. Malignant pleural mesothelioma: CT manifestations in 50 cases. AJR Am J Roentgenol. 1990; 155(5): 965-9. (IV)
- 3)Okten F, Köksal D, Onal M, et al. Computed tomography findings in 66 patients with malignant pleural mesothelioma due to environmental exposure to asbestos. Clin Imaging. 2006; 30(3): 177-80. (IV)
- 4)Leung AN, Müller NL, Miller RR. CT in differential diagnosis of diffuse pleural disease. AJR Am J Roentgenol. 1990; 154(3): 487-92. (IV)
- 5)Yilmaz U, Polat G, Sahin N, et al. CT in differential diagnosis of benign and malignant pleural disease. Monaldi Arch Chest Dis. 2005; 63(1): 17-22. (IV)
- 6)Metintas M, Ucgun I, Elbek O, et al. Computed tomography features in malignant pleural mesothelioma and other commonly seen pleural diseases. Eur J Radiol. 2002; 41(1): 1-9. (IV)
- 7)Falaschi F, Battolla L, Mascalchi M, et al. Usefulness of MR signal intensity in distinguishing benign from malignant pleural disease. AJR Am J Roentgenol. 1996; 166(4): 963-8. (IV)
- 8)Hierholzer J, Luo L, Bittner RC, et al. MRI and CT in the differential diagnosis of pleural disease. Chest. 2000; 118(3): 604-9. (IV)
- 9)Boraschi P, Neri S, Braccini G, et al. Magnetic resonance appearance of asbestos-related benign and malignant pleural diseases. Scand J Work Environ Health. 1999; 25(1): 18-23. (IV)
- 10)Knuuttila A, Kivisaari L, Kivisaari A, et al. Evaluation of pleural disease using MR and CT. With special reference to malignant pleural mesothelioma. Acta Radiol. 2001; 42(5): 502-7. (IV)
- 11)Coolen J, De Keyzer F, Nafteux P, et al. Malignant pleural disease: diagnosis by using diffusion-weighted and dynamic contrast-enhanced MR imaging--initial experience. Radiology. 2012; 263(3): 884-92. (IV)
- 12)Carretta A, Landoni C, Melloni G, et al. 18-FDG positron emission tomography in the evaluation of malignant pleural diseases―a pilot study. Eur J Cardiothorac Surg. 2000; 17(4): 377-83. (IV)
- 13)Duysinx B, Nguyen D, Louis R, et al. Evaluation of pleural disease with 18-fluorodeoxyglucose positron emission tomography imaging. Chest. 2004; 125(2): 489-93. (IV)
- 14)Yamamoto Y, Kameyama R, Togami T, et al. Dual time point FDG PET for evaluation of malignant pleural mesothelioma. Nucl Med Commun. 2009; 30(1): 25-9. (IV)
- 15)Mavi A, Basu S, Cermik TF, et al. Potential of dual time point FDG-PET imaging in differentiating malignant from benign pleural disease. Mol Imaging Biol. 2009; 11(5): 369-78. (IV)
- 16)Kurata S, Ishibashi M, Azuma K, et al. Preliminary study of positron emission tomography/computed tomography and plasma osteopontin levels in patients with asbestos-related pleural disease. Jpn J Radiol. 2010; 28(6): 446-52. (IV)
- 17)Yildirim H, Metintas M, Entok E, et al. Clinical value of fluorodeoxyglucose-positron emission tomography/computed tomography in differentiation of malignant mesothelioma from asbestos-related benign pleural disease: an observational pilot study. J Thorac Oncol. 2009; 4(12): 1480-4. (IV)
- 18)Orki A, Akin O, Tasci AE, et al. The role of positron emission tomography/computed tomography in the diagnosis of pleural diseases. Thorac Cardiovasc Surg. 2009; 57(4): 217-21. (IV)
- 19)Elboga U, Yllmaz M, Uyar M, et al. The role of FDG PET-CT in differential diagnosis of pleural pathologies. Rev Esp Med Nucl Imagen Mol. 2012; 31(4): 187-91. (IV)
- 20)Abe Y, Tamura K, Sakata I, et al. Clinical implications of 18F-fluorodeoxyglucose positron emission tomography/computed tomography at delayed phase for diagnosis and prognosis of malignant pleural mesothelioma. Oncol Rep. 2012; 27(2): 333-8. (IV)
- 21)Porcel JM, Hernández P, Martínez-Alonso M, et al. Accuracy of fluorodeoxyglucose-PET imaging for differentiating benign from malignant pleural effusions: a meta-analysis. Chest. 2015; 147(2): 502-12. (I)
